Learning Objectives
Master the classification and pathophysiology of Obstructive Lung Diseases. Distinguish between Chronic Bronchitis, Emphysema, Asthma, and Bronchiectasis based on clinical criteria, microscopic findings, and radiological evidence for the USMLE Step 1.
1. Core Pathophysiology: The Obstructive Pattern
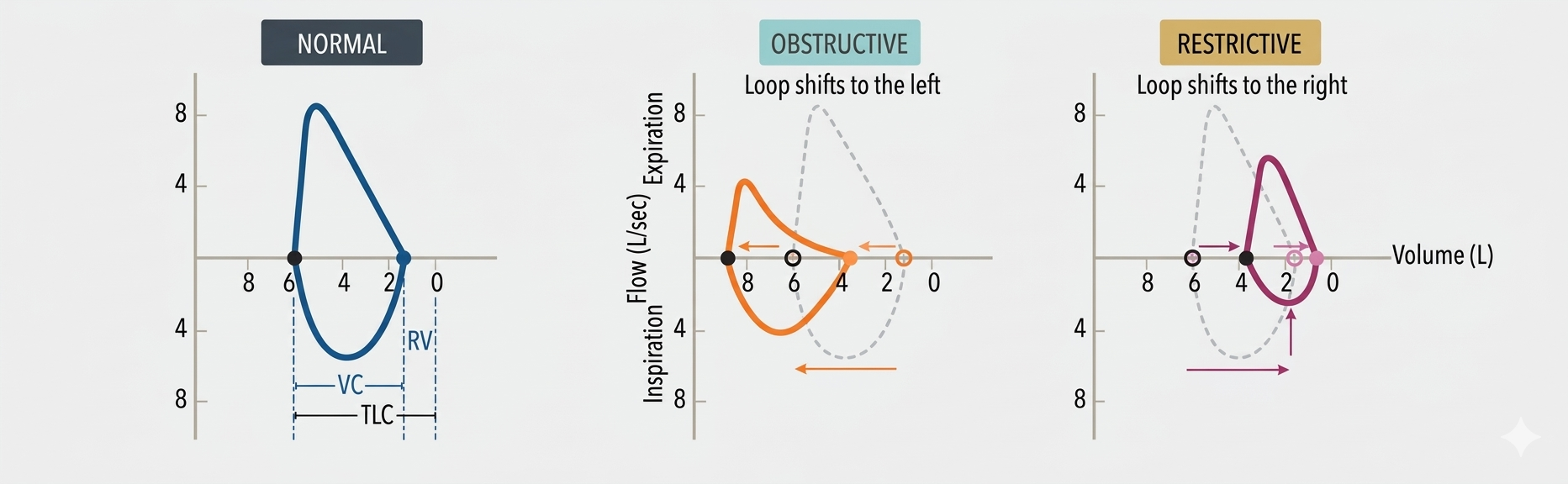
All obstructive diseases share a common mechanism: obstruction of airflow, especially during expiration. This leads to air trapping in the lungs due to premature airway closure at high lung volumes. Latex
| Parameter | Change | Mechanism |
|---|---|---|
 |
Markedly Decreased ( ) ) |
Increased resistance to expiratory flow. |
 |
Decreased ( ) ) |
Air trapping limits the total volume exhaled. |
 |
Decreased (< 70%) | falls much more than . |
| RV, FRC, TLC | Increased ( ) ) |
Hyperinflation and residual air volume. |
2. Chronic Bronchitis (“Blue Bloater”)
| Category | Details |
|---|---|
| Diagnosis | Clinical: Productive cough for ≥ 3 months in ≥ 2 consecutive years. |
| Mechanism | Hypertrophy and hyperplasia of mucus-secreting glands in bronchi. |
| Pathology | Reid Index > 50%; squamous metaplasia of respiratory epithelium. |
| Presentation | Cyanosis (shunting), wheezes, crackles, and secondary polycythemia. |
3. Emphysema (“Pink Puffer”)
Shutterstock Explore
| Type | Association | Location |
|---|---|---|
| Centriacinar | Smoking | Upper lobes; spares distal alveoli. |
| Panacinar |  -antitrypsin deficiency -antitrypsin deficiency |
Lower lobes; affects the entire acinus. |
| Physiology | Compliance, Recoil |
 due to alveolar wall destruction. due to alveolar wall destruction. |
4. Asthma
| Feature | Details |
|---|---|
| Mechanism | Reversible bronchoconstriction; Type I hypersensitivity; muscle hypertrophy. |
| Triad | Samter’s Triad: Asthma, Nasal polyps, ASA/NSAID sensitivity. |
| Sputum | Curschmann spirals (mucus plugs); Charcot-Leyden crystals (eosinophils). |
| Diagnosis | Spirometry (reversible) or Methacholine challenge. |
5. Bronchiectasis
| Factor | Description |
|---|---|
| Pathology | Permanently dilated airways from chronic inflammation/infection. |
| Symptoms | Chronic cough with copious purulent sputum; recurrent infections. |
| Imaging | Airway dilation and bronchial thickening (“tram-tracking”). |
| Causes | Cystic Fibrosis, Kartagener syndrome, ABPA, and Obstruction. |
Activity:
Activity
High-Yield Clinical Pearls:
- Protease Imbalance: In emphysema, the alveolar destruction is driven by an imbalance where elastase (from neutrophils) outweighs antiproteases.
- Blue vs. Pink: Bronchitis patients are “blue” due to early hypoxemia/cyanosis; Emphysema patients are “pink” as they hyperventilate to maintain oxygenation.
- The Reid Index: Specifically measures the gland-to-wall ratio in the bronchus, not the bronchiole.
You must be logged in to post a comment.