Learning Objectives
Master the classification and pathophysiology of Restrictive Lung Diseases. Distinguish between extrapulmonary (altered mechanics) and pulmonary (parenchymal) causes, and understand the changes in pulmonary function tests (PFTs) and gas exchange parameters for the USMLE Step 1.
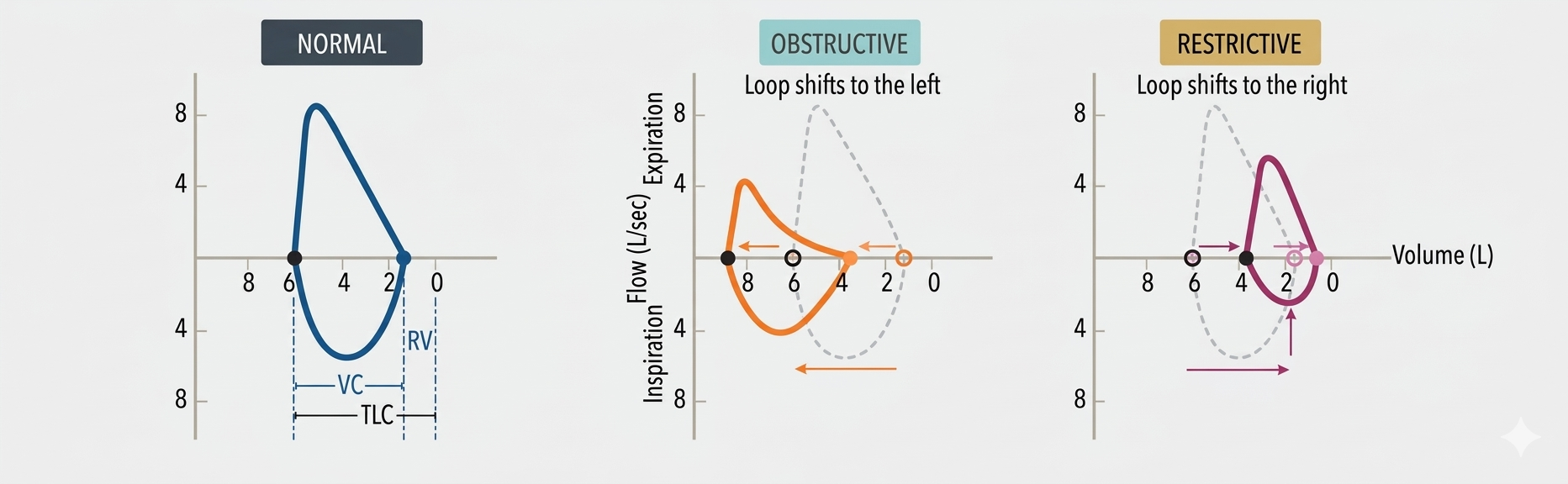
1. Core Pathophysiology: The Restrictive Pattern
Restrictive lung diseases are characterized by reduced lung volumes. The lungs are often described as “stiff,” with decreased compliance, making it difficult to expand the chest or lungs during inspiration. Latex
| Parameter | Change | Mechanism |
|---|---|---|
 and and  |
Decreased ( ) ) |
Inability to fully expand the lungs or chest wall. |
 |
Normal or Increased ( ) ) |
 decreases proportionately to (or less). decreases proportionately to (or less). |
| Clinical Signs | Short, shallow breaths | “Velcro-type” crackles on auscultation. |
2. Extrapulmonary: Altered Respiratory Mechanics
In these conditions, the lungs themselves are healthy, but the “pump” (muscles or chest wall) is failing. This results in restriction without affecting the lung tissue’s ability to exchange gas.
| Category | Examples | Gas Exchange Indicators |
|---|---|---|
| Neuromuscular | Polio, Myasthenia Gravis, Guillain-Barré, ALS. | Normal  Normal A-a gradient Normal A-a gradient |
| Chest Wall | Scoliosis, Morbid obesity. |
3. Pulmonary: Interstitial Lung Diseases (ILD)
These involve direct damage to the lung parenchyma, leading to inflammation and fibrosis. This increases the thickness of the blood-gas barrier, impairing diffusion.
| Disease | Distinctive Features | Gas Exchange Indicators |
|---|---|---|
| Sarcoidosis | Bilateral hilar lymphadenopathy; Noncaseating granulomas; ACE;  . . |
Decreased Increased A-a gradient |
| Pneumoconioses | Asbestosis, Silicosis, Coal workers’ pneumoconiosis. | |
| Idiopathic Fibrosis | Chronic scarring of unknown etiology; “Honeycomb” lung. | |
| Drug Toxicity | Bleomycin, Busulfan, Amiodarone, Methotrexate. |
4. Radiation-Induced Lung Injury
Radiation damage is mediated by the release of proinflammatory cytokines (TNF-
| Phase | Timeline | Clinical Features |
|---|---|---|
| Acute Pneumonitis | 3–12 weeks post-radiation | Exudative phase; dry cough, dyspnea, low-grade fever. |
| Radiation Fibrosis | 6–12 months post-radiation | Chronic scarring; progressive restrictive defect. |
Activity:
Activity
High-Yield Clinical Pearls:
- The
- Sarcoidosis Granulomas: Remember that the macrophages in these noncaseating granulomas produce 1-
- A-a Gradient: This is usually increased in ILD due to the physical barrier of fibrosis slowing oxygen diffusion from the alveolus to the capillary.
You must be logged in to post a comment.