Learning Objectives
Master the interpretation of Flow-Volume Loops and pulmonary function test (PFT) parameters. Distinguish between Obstructive and Restrictive lung disease patterns, and understand the shifts in lung volumes (TLC, FRC, RV) for the USMLE Step 1.
1. Anatomy of the Flow-Volume Loop
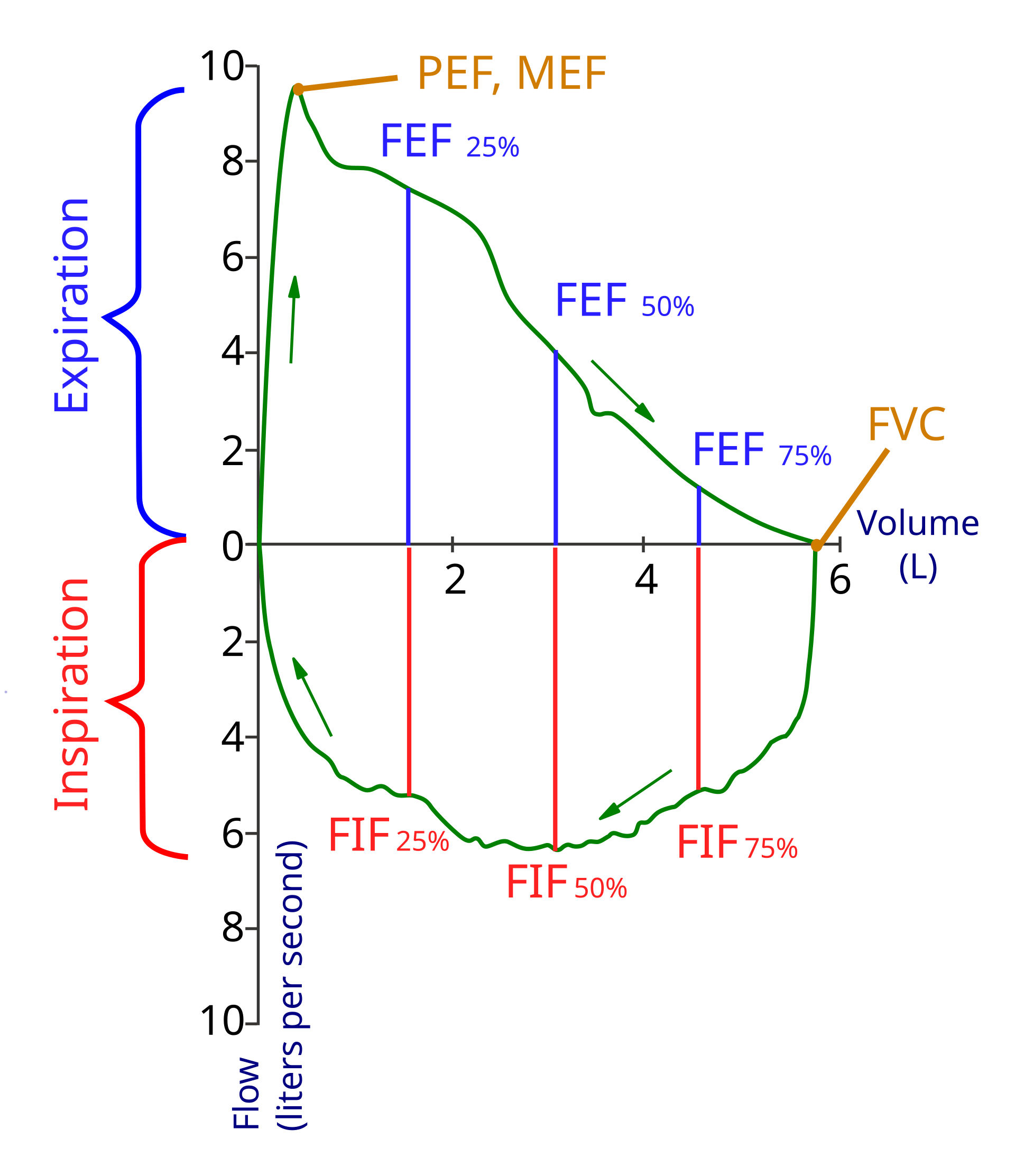
A flow-volume loop plots the rate of airflow (L/sec) against the total volume of air in the lungs. The top half represents expiration (active/effort-dependent), and the bottom half represents inspiration.
| Point on Loop | Definition |
|---|---|
| Leftmost Point | TLC (Total Lung Capacity): Maximum air inspired. |
| Rightmost Point | RV (Residual Volume): Air remaining after maximal expiration. |
| Horizontal Width | FVC (Forced Vital Capacity): The total volume of air exhaled. |
2. Obstructive Lung Disease Pattern
Obstructive diseases (e.g., COPD, Asthma) are characterized by difficulty getting air OUT. This leads to air trapping and hyperinflation.
| Parameter | Change | Why? |
|---|---|---|
| Loop Shape | “Scooped-out” expiration | Premature airway closure during exhalation. |
| Loop Position | Shifts to the LEFT | Increased TLC, FRC, and RV due to air trapping. |
 Ratio Ratio |
Decreased (< 70%) |  drops significantly more than $FVC$. drops significantly more than $FVC$. |
3. Restrictive Lung Disease Pattern
Restrictive diseases (e.g., Pulmonary Fibrosis, Obesity) are characterized by difficulty getting air IN. The lungs are small and “stiff.”
| Parameter | Change | Why? |
|---|---|---|
| Loop Shape | Miniature/Narrow version | Overall reduction in all lung volumes. |
| Loop Position | Shifts to the RIGHT | Decreased TLC and RV. |
| Ratio |
Normal or Increased | Both and  decrease proportionately. decrease proportionately. |
Activity:
High-Yield Clinical Pearls:
- The Left Shift: If the loop is “fat” and moves left, it’s Obstructive (think big, air-filled lungs).
- The Right Shift: If the loop is “thin” and moves right, it’s Restrictive (think small, scarred lungs).
- Upper Airway Obstruction: Look for a flattening of both the inspiratory and expiratory limbs (the “box” shape).
You must be logged in to post a comment.