Learning Objectives
Master the concept of Work of Breathing (WOB). Understand the balance between elastic and resistive work, and how patients with Obstructive vs. Restrictive lung diseases automatically adjust their respiratory rate and tidal volume to minimize energy expenditure for the USMLE Step 1.
1. Components of Respiratory Work
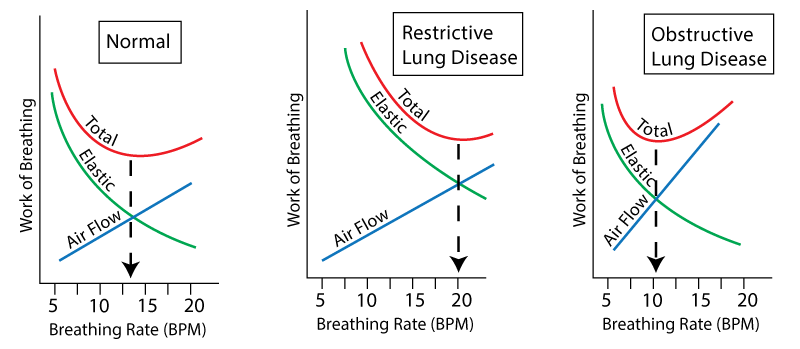
Work of breathing is the energy required to overcome two major opposing forces: Elastic Recoil and Airway Resistance.
| Type of Work | Force to Overcome | Determining Factor |
|---|---|---|
| Elastic Work | The “stiffness” of the lung/chest wall. | Correlates with Tidal Volume ( ). Larger breaths require more elastic work. ). Larger breaths require more elastic work. |
| Flow-Resistive Work | Friction of air moving through the tubes. | Correlates with Respiratory Rate (RR). Faster breathing increases turbulence and resistance. |
2. Clinical Adaptations in Disease
Patients naturally adopt a breathing pattern that minimizes the Total Work. The “sweet spot” on the graph shifts depending on the underlying pathology.
| Disease Category | Primary Burden | Compensatory Pattern |
|---|---|---|
| Restrictive | High Elastic Resistance (Stiff lungs). | ↑ RR, ↓ (Rapid, shallow breaths). Small breaths avoid stretching stiff lungs. |
| Obstructive | High Airway Resistance (Narrow tubes). | ↓ RR, ↑ (Slow, deep breaths). Slow breathing reduces frictional resistance. |
3. Energy Expenditure and Mechanics
The body aims for maximum efficiency. In healthy states, the work required for ventilation is minimal, but this changes drastically with disease.
| Parameter | Physiological Goal | Clinical Implication |
|---|---|---|
| Total Work | Minimize  consumption of respiratory muscles. consumption of respiratory muscles. |
Normally, < 5% of total ; can rise to > 30% in respiratory failure. |
| Equation |  |
Reflected by the area within a pressure-volume loop. |
| Optimal RR | Determined by the “inflection point” of the work curves. | Shifted right (higher RR) in restrictive; shifted left (lower RR) in obstructive. |
Activity:
High-Yield Clinical Pearls:
- The Restrictive Logic: Think of a fibrotic lung like a thick rubber band. It is difficult to stretch, so taking many small, quick breaths is more efficient than fighting the elastic recoil of a deep breath.
- The Obstructive Logic: Think of asthma or COPD like breathing through a straw. High-velocity air creates more turbulence/resistance. Taking slow, deep breaths keeps the flow laminar and reduces the work of friction.
- Respiratory Failure: When the work required to breathe exceeds the energy available to the muscles, the patient will develop hypercapnic respiratory failure.
You must be logged in to post a comment.