Learning Objectives
- Identify the nerve roots and sensory/motor distributions of the lower extremity.
- Correlate specific surgical and traumatic injuries with clinical presentations (e.g., foot drop, Trendelenburg).
- Apply the PED and TIP mnemonics to distinguish peroneal and tibial nerve functions.
- Recognize the anatomical landmarks for pudendal nerve blocks and intramuscular injections.
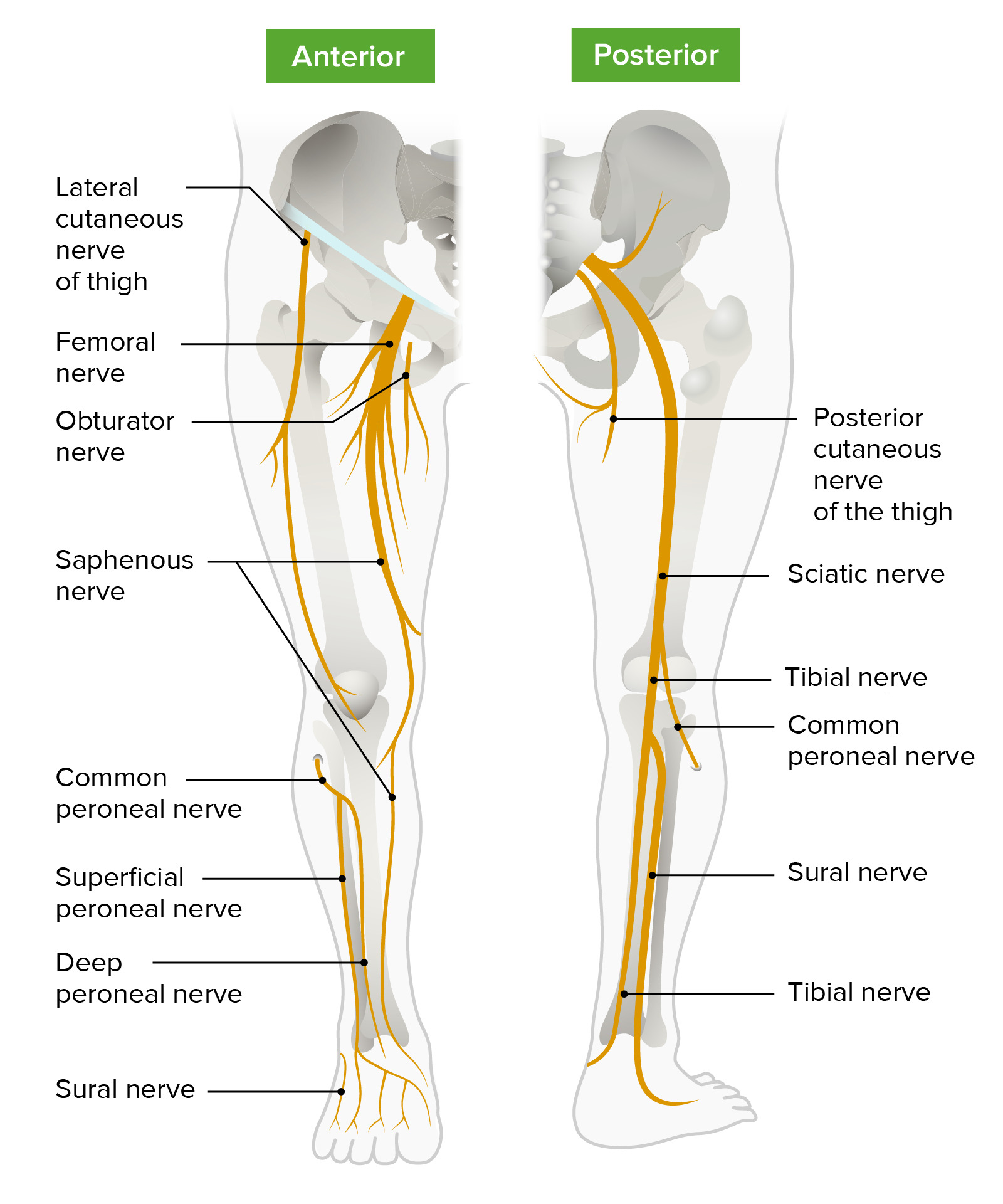
1. Nerves of the Pelvis and Thigh
These nerves are frequently injured during abdominal or pelvic procedures.
- Iliohypogastric (T12-L1): Often injured during inguinal hernia repair. Leads to burning pain radiating to the suprapubic region.
- Genitofemoral (L1-L2): Injured in laparoscopic surgery. Results in an absent cremasteric reflex and decreased sensation on the upper medial thigh.
- Lateral Femoral Cutaneous (L2-L3): Compressed by tight clothing or obesity (Meralgia Paresthetica). Causes burning pain in the anterolateral thigh; no motor deficit.
- Obturator (L2-L4): Injured in pelvic surgery. Leads to decreased thigh adduction and medial thigh sensation.
- Femoral (L2-L4): Injured by pelvic fractures or psoas abscesses. Results in loss of knee extension and a decreased patellar reflex.
Activity:
2. The Sciatic Branches: PED and TIP
The sciatic nerve (L4-S3) splits into the common peroneal and tibial nerves. Their deficits are high-yield for gait analysis.
| Nerve | Injury Site | Clinical Presentation |
|---|---|---|
| Common Peroneal (L4-S2) | Fibular neck fracture or compression. | Foot Drop; loss of eversion/dorsiflexion; “steppage gait.” (PED) |
| Tibial (L4-S3) | Knee trauma or Baker cyst. | Inability to curl toes; loss of sensation on sole; cannot stand on TIPtoes. (TIP) |
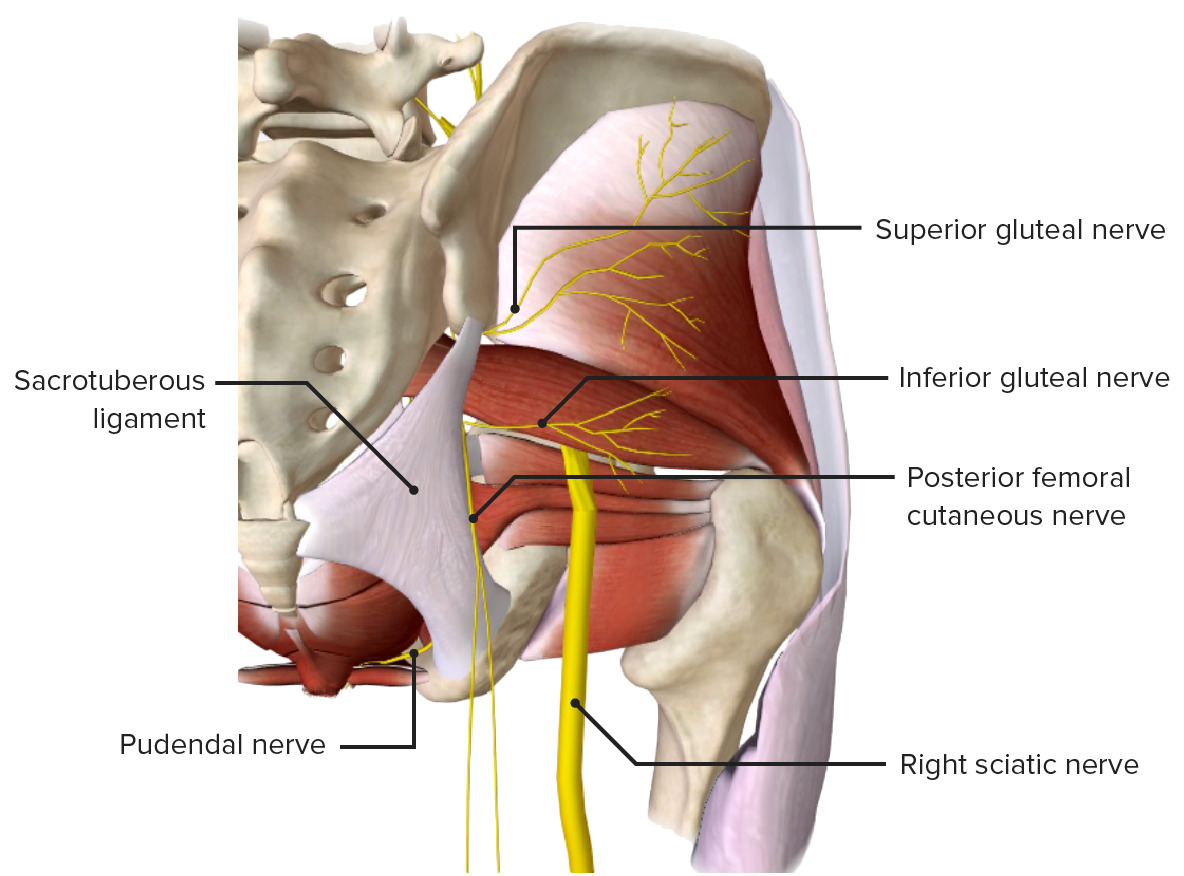
3. Gluteal and Pudendal Nerves
These nerves control the “power” movements of the hip and pelvic floor functions.
- Superior Gluteal (L4-S1): Injured by injections in the superomedial gluteal quadrant.
- Trendelenburg Sign: The pelvis tilts because the weight-bearing leg cannot abduct. The lesion is contralateral to the side of the hip drop.
- Inferior Gluteal (L5-S2): Injured by posterior hip dislocation. Causes difficulty climbing stairs or rising from a seat (loss of hip extension).
- Pudendal (S2-S4): Injured by childbirth or prolonged cycling.
- Clinical: Perineal anesthesia; fecal/urinary incontinence. The ischial spine is the landmark for a pudendal block.
Clinical Notes & Corrections:
- Safe Injection Site: To avoid the superior gluteal and sciatic nerves, use the superolateral quadrant of the gluteus.
- Meralgia Paresthetica: This condition only affects sensation. If a patient presents with thigh pain and weakness, look toward the femoral nerve instead.
- Sciatic Nerve: Posterior hip dislocations are a classic board question for both Sciatic and Inferior Gluteal nerve injuries.
You must be logged in to post a comment.