Learning Objectives
Master the structural and functional anatomy of the Placenta. Distinguish between the fetal and maternal layers and understand the endocrine and immunological role of the Syncytiotrophoblast for the USMLE Step 1.
1. Fetal Component: The Trophoblast Layers
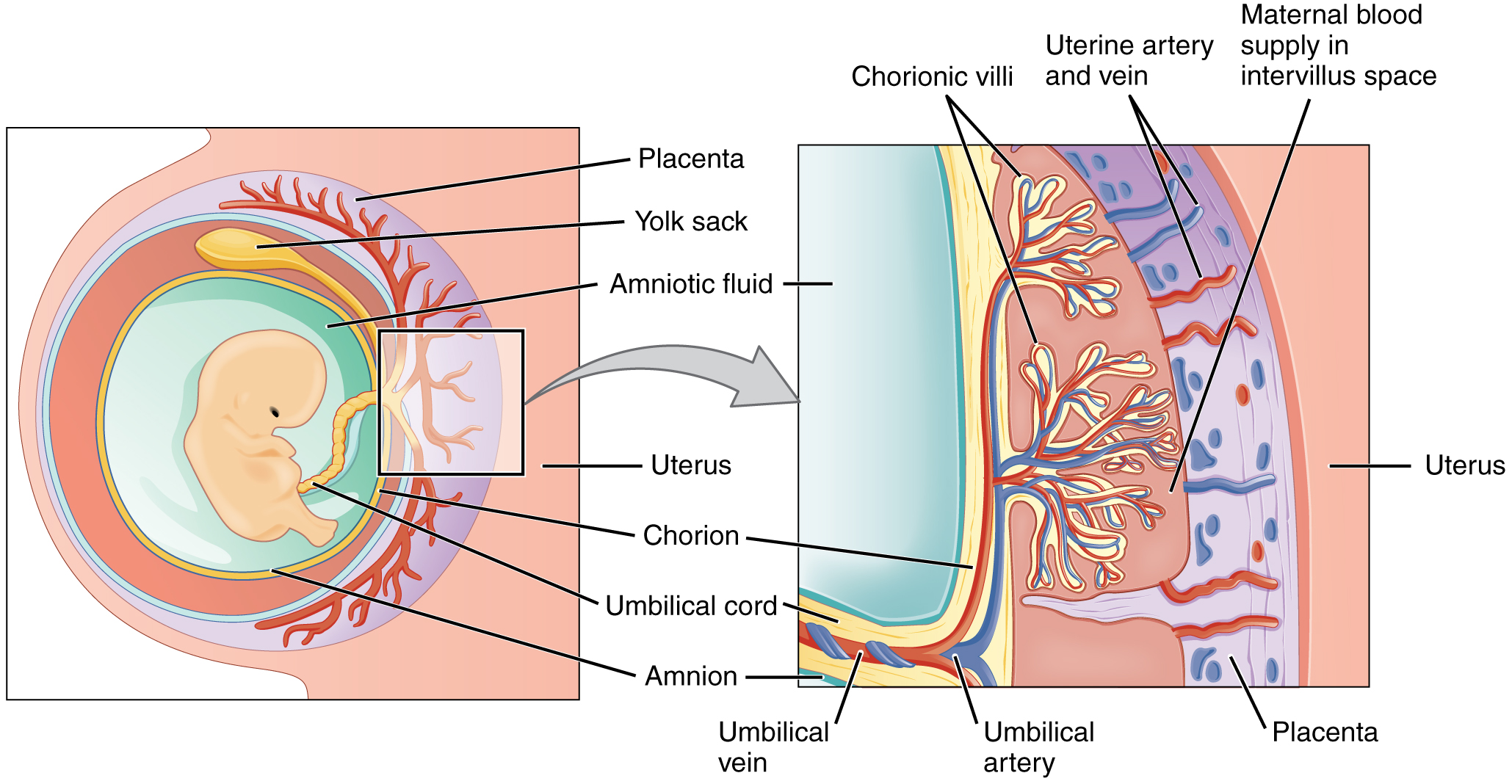
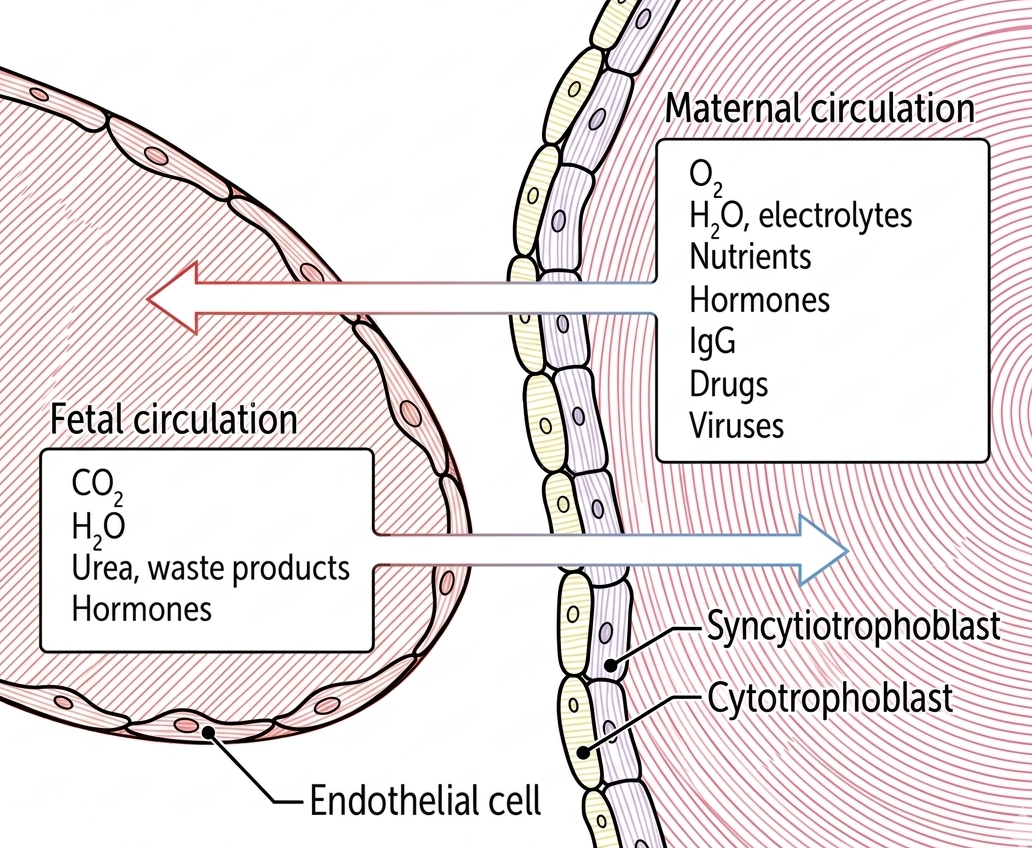
The fetal portion of the placenta is derived from the chorionic villi. It consists of two distinct layers with specialized functions.
| Layer | Description | Key Clinical Function |
|---|---|---|
| Cytotrophoblast | Inner layer of chorionic villi. | Cyto creates cells; it serves as the stem cell reservoir for the outer layer. |
| Syncytiotrophoblast | Outer layer of chorionic villi. | Synthesizes hCG; lacks MHC I expression to avoid maternal immune attack. |
2. Maternal Component: Decidua Basalis
The maternal side of the placenta is formed by the modified endometrium, providing the environment for nutrient exchange.
| Structure | Origin/Function |
|---|---|
| Decidua basalis | Derived from the maternal endometrium. |
| Lacunae | Spaces filled with maternal blood where the fetal villi are bathed. |
3. Gas and Nutrient Exchange
The placenta serves as the lungs, kidneys, and digestive tract for the fetus.
| Direction | Materials Transferred |
|---|---|
| Maternal to Fetal | O₂, H₂O, electrolytes, nutrients, hormones, IgG, drugs, and viruses. |
| Fetal to Maternal | CO₂, H₂O, urea, waste products, and hormones. |
Activity
High-Yield Clinical Pearls:
- HCG & LH: Because hCG is structurally similar to LH, it can maintain the corpus luteum and progesterone production during the first trimester.
- Immune Privilege: The Syncytiotrophoblast lacks MHC I, which is a key reason why the mother’s T-cells don’t recognize the fetus as “foreign.”
- Antibody Transfer: Only IgG crosses the placenta. IgA, IgM, IgE, and IgD do not cross.
You must be logged in to post a comment.