Learning Objectives
- Explain the pathophysiology of Osteoporosis, specifically the imbalance between osteoblasts and osteoclasts.
- Identify the diagnostic criteria (T-score) and screening guidelines for bone mineral density.
- List key risk factors, including hormonal, lifestyle, and pharmacological causes.
- Recognize the clinical presentation of vertebral compression fractures and other common fracture sites.
1. Pathophysiology and Bone Loss
Osteoporosis is characterized by a reduction in both trabecular (spongy) and cortical bone mass. Crucially, the bone that remains is normally mineralized—there is just less of it.
- Mechanism: Primarily due to increased bone resorption. This is often triggered by decreased estrogen levels (menopause), which normally limits osteoclast activity.
- Laboratory Values: A high-yield Step 1 fact is that Serum Calcium, Phosphate, and PTH are typically NORMAL in primary osteoporosis.
- Secondary Causes:
- Drugs: Long-term Corticosteroids, Anticonvulsants, Heparin, and PPIs.
- Conditions: Hyperparathyroidism, Multiple Myeloma, Malabsorption, and Hyperthyroidism.
- Environment: Prolonged microgravity (space travel) or immobilization.
2. Diagnosis and Screening
Osteoporosis is often “silent” until a fracture occurs. Screening is essential for early detection.
- DEXA Scan: Dual-energy X-ray absorptiometry at the lumbar spine, total hip, and femoral neck.
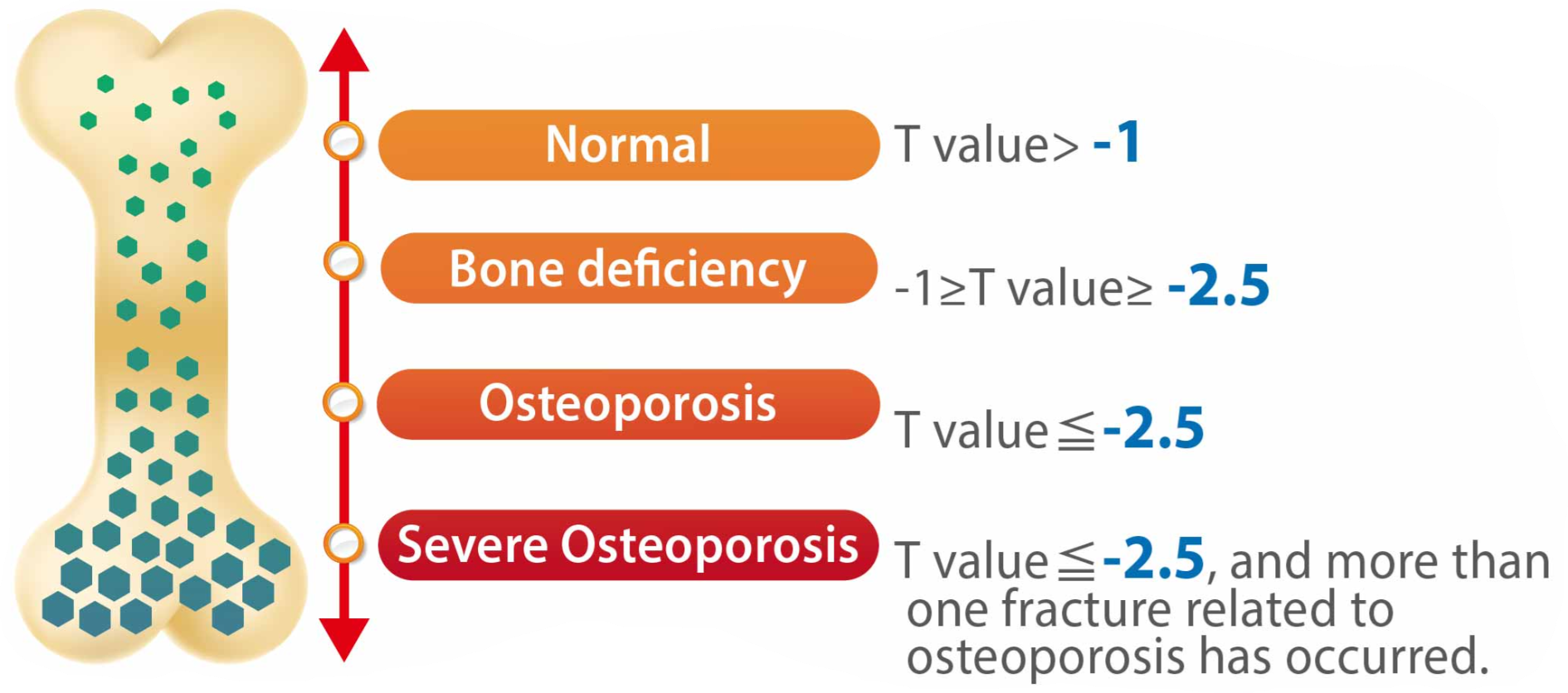
- T-score
-2.5: Diagnostic for Osteoporosis. (T-score between -1.0 and -2.5 is Osteopenia).
- Fragility Fracture: A diagnosis can be made regardless of T-score if a patient suffers a fracture from minimal trauma (e.g., falling from standing height).
- Screening: Recommended for all females
65 years old.
3. Clinical Consequences
Loss of bone density leads to characteristic skeletal changes and “fragility” fractures.
- Vertebral Compression Fracture: Presents with acute back pain, loss of height, and Kyphosis (Dowager’s hump).
- Colles Fracture: Fracture of the distal radius (common in FOOSH injuries).
- Hip Fractures: Specifically of the femoral neck; associated with high morbidity and mortality in the elderly.
Pharmacology Summary (High Yield):
- Bisphosphonates: First-line; inhibit osteoclasts (side effect: corrosive esophagitis).
- Teriparatide: Recombinant PTH; anabolic (builds bone) if given in pulsatile/intermittent doses.
- Denosumab: Monoclonal antibody against RANKL (mimics OPG).
- SERMs (Raloxifene): Estrogen agonist in bone, antagonist in breast/uterus.
Activity: Osteoporosis vs. Other Bone Diseases
Quick Mnemonics:
Osteoporosis: Porous bone (the labs are fine, the Ports are empty).
DEXA: Density Exam for X-ray Analysis.
Osteoporosis: Porous bone (the labs are fine, the Ports are empty).
DEXA: Density Exam for X-ray Analysis.
You must be logged in to post a comment.