Learning Objectives
- Identify the anatomical compartments involved in a psoas abscess.
- Differentiate between the primary microbiology (S. aureus vs. M. tuberculosis).
- Recognize high-yield clinical signs (Psoas sign) and risk factors (Crohn disease).
- Analyze imaging findings and first-line treatment protocols.
1. Pathophysiology and Spread
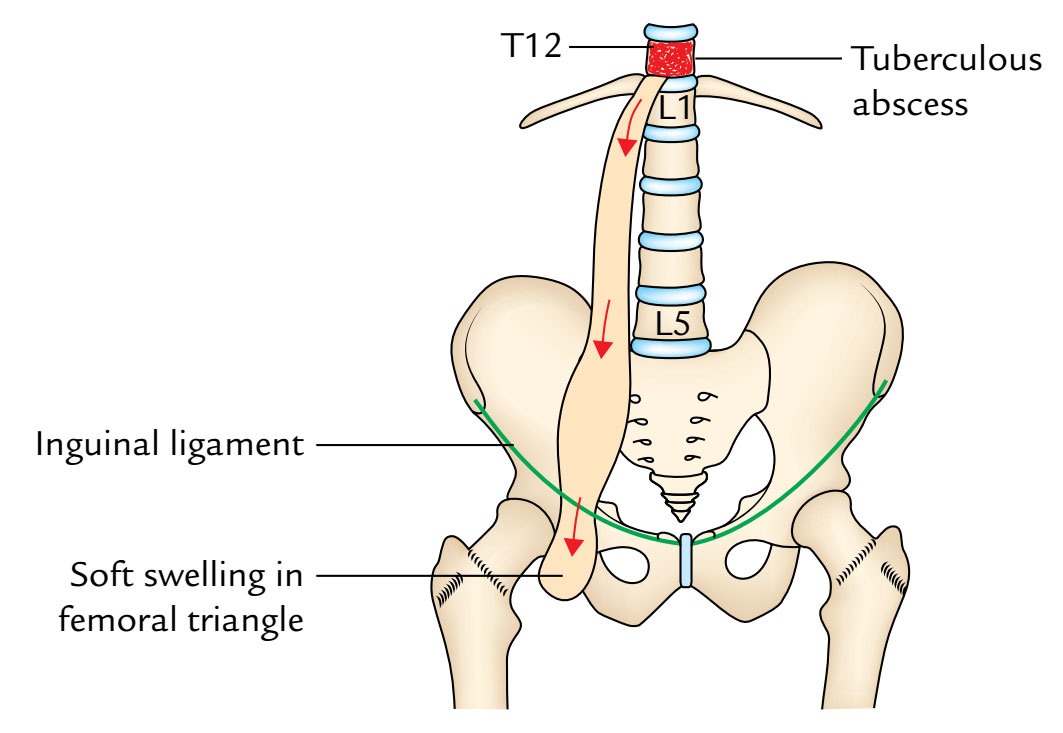
A psoas abscess is a collection of pus within the iliopsoas muscle group. Because the psoas muscle originates from the T12–L5 vertebrae and inserts into the lesser trochanter, it provides a direct “conduit” for infection to travel from the spine to the groin.
- Hematogenous Spread: Bacteria travel through the blood to the muscle.
- Contiguous Spread: Infection spreads from adjacent structures:
- Vertebral Osteomyelitis / Pott Disease (Tuberculous spondylitis).
- Renal: Pyelonephritis or perinephric abscess.
- Gastrointestinal: Crohn disease (due to the proximity of the psoas to the ileum/appendix).
2. Clinical Presentation
Diagnosis is often delayed because symptoms can be vague or mimic other abdominal/hip pathologies.
- The “Classic” Triad: Fever, flank/back pain, and a palpable inguinal mass.
- Psoas Sign: Abdominal or hip pain exacerbated by passive extension of the hip. This stretches the inflamed psoas muscle.
- Microbiology:
- Most Common: Staphylococcus aureus.
- Secondary: Mycobacterium tuberculosis (especially in endemic areas or immunocompromised patients).
3. Diagnosis and Management
| Modality | Key Finding |
|---|---|
| Imaging (CT/MRI) | Hypodense lesion (fluid collection) within the muscle plane. CT is the gold standard. |
| Laboratory | Leukocytosis, elevated ESR/CRP. |
| Treatment | Percutaneous or surgical abscess drainage + targeted antibiotic therapy. |
Clinical Notes & Step 1 Pearls:
- Crohn Disease Link: If a patient with a history of Crohn’s presents with new-onset hip pain and fever, suspect a psoas abscess.
- Pott Disease: In a patient with TB, the psoas abscess is often called a “cold abscess” because it lacks the classic warmth and redness of an acute pyogenic infection.
- Differential: Must be distinguished from appendicitis (which can also have a positive psoas sign if the appendix is retrocecal).
Activity: Psoas Abscess Diagnostic Logic
Quick Mnemonics:
Psoas Sign: Passive Extension = Pain.
S. aureus: Usually the “Gold” standard for skin/muscle abscesses.
You must be logged in to post a comment.