Learning Objectives
- Differentiate between Medial and Lateral Epicondylitis based on clinical presentation.
- Correlate specific wrist movements (flexion vs. extension) with the affected elbow landmark.
- Identify the anatomical structures involved in common overuse injuries of the elbow.
1. Medial (Golfer’s) Elbow
Medial epicondylitis is an overuse injury affecting the common flexor tendon that attaches to the medial epicondyle of the humerus.
- Mechanism: Repetitive wrist flexion (e.g., golfing, throwing, or manual labor involving a strong grip).
- Presentation: Pain and tenderness localized near the medial epicondyle. Pain may worsen with resisted wrist flexion or forearm pronation.
- Anatomy: Primarily involves the pronator teres and flexor carpi radialis.
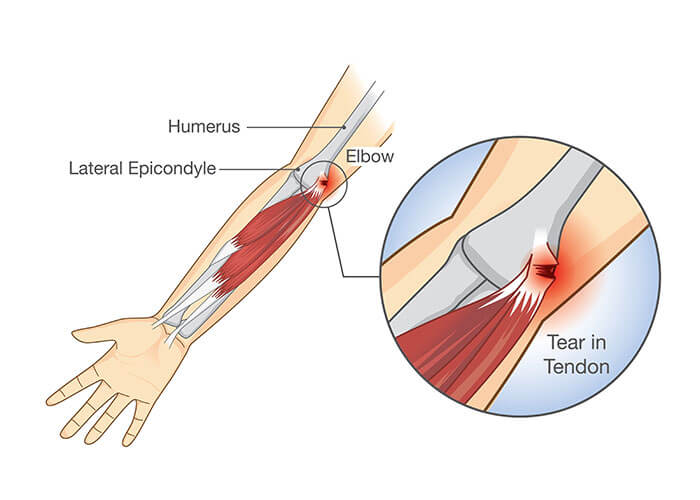
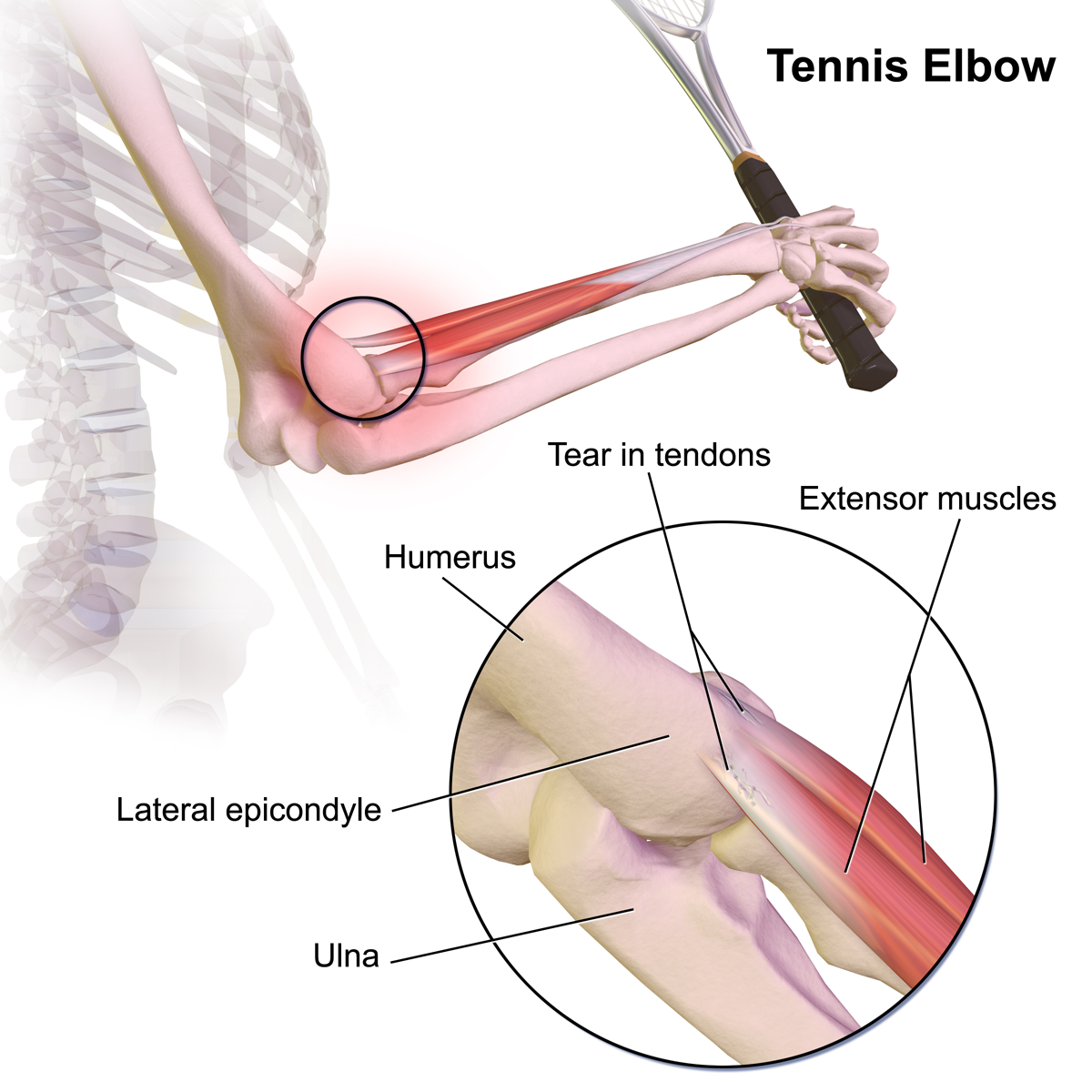
2. Lateral (Tennis) Elbow
Lateral epicondylitis is the most common overuse injury of the elbow, affecting the common extensor origin.
- Mechanism: Repetitive wrist extension (e.g., tennis backhand shots, typing, or repetitive use of a screwdriver).
- Presentation: Pain and tenderness over the lateral epicondyle. Pain is often reproducible with resisted wrist extension while the elbow is in full extension.
- Anatomy: Most commonly involves the extensor carpi radialis brevis (ECRB).
Clinical Notes & Step 1 Pearls:
- Terminology: Although often called “epicondylitis,” these are usually tendinopathies (chronic degenerative changes) rather than acute inflammatory “itis” conditions.
- Ulnar Nerve: In medial epicondylitis, be aware of the ulnar nerve which sits in the cubital tunnel just posterior to the medial epicondyle; chronic inflammation can occasionally lead to ulnar neuropathy.
- Radial Nerve: Lateral elbow pain can sometimes mimic radial tunnel syndrome, where the deep branch of the radial nerve is compressed.
Activity: Elbow Tendinopathy Identification
Quick Mnemonics:
Medial: Medial = Manual Flexion (Golfer/Flexor).
Lateral: Lateral = Long Extension (Tennis/Extensor).
You must be logged in to post a comment.