Learning Objectives
- Explain the pathophysiology of disc herniation (nucleus pulposus through annulus fibrosus).
- Master the “N+1” Rule for posterolateral herniations in the lumbar spine.
- Differentiate between L4, L5, and S1 radiculopathies based on motor, sensory, and reflex deficits.
- Identify key physical exam maneuvers for nerve root tension.
1. Pathophysiology: The Posterolateral Slip
Intervertebral discs consist of a jelly-like nucleus pulposus surrounded by a fibrous annulus fibrosus.
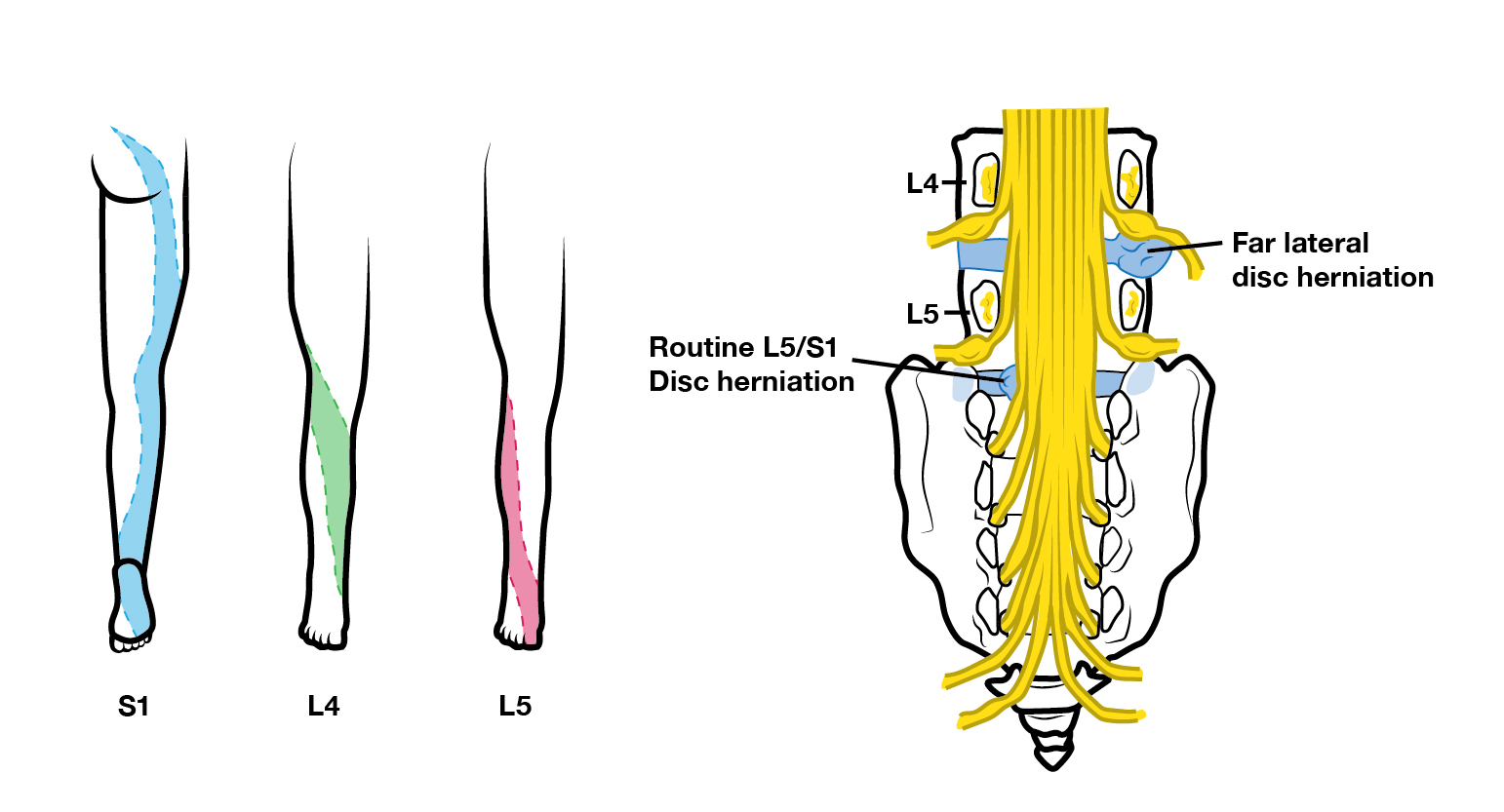
- Mechanism: The nucleus pulposus herniates posterolaterally.
- Why Posterolateral? The Posterior Longitudinal Ligament is much thinner than the Anterior Longitudinal Ligament, making the back side of the disc the path of least resistance.
- The “N+1” Rule: In the lumbar spine, a posterolateral herniation typically affects the traversing nerve root (the one below the level of herniation). For example, an L4-L5 disc herniation hits the L5 nerve root.
2. Clinical Findings by Nerve Root
| Nerve Root | Disc Level | Motor Deficit | Reflex & Sensory |
|---|---|---|---|
| L4 | L3–L4 | Weakness of Knee Extension: Difficulty with stairs. | ↓ Patellar Reflex; Sensation over the medial leg/malleolus. |
| L5 | L4–L5 | Weakness of Dorsiflexion; Difficulty Heel Walking. | Sensation over the dorsal foot and webspace of the 1st/2nd toes. |
| S1 | L5–S1 | Weakness of Plantar Flexion: Difficulty with toe walking. | ↓ Achilles Reflex: Sensation over the lateral foot/little toe. |
3. Physical Exam: Tension Signs
These maneuvers stretch the nerve roots to see if they elicit radicular pain (pain radiating down the leg).
- Straight Leg Raise (SLR): High sensitivity for L5/S1 herniation. Pain elicited between 30° 70°.
- Contralateral SLR: Lifting the unaffected leg causes pain in the affected leg. This is highly specific for a disc herniation.
- Reverse SLR (Femoral Stretch): Assesses upper lumbar roots (L2–L4). The patient is prone, and the knee is flexed while the hip is extended.
Activity:
Clinical Notes & Corrections:
- Cauda Equina Syndrome: A surgical emergency! Look for “Saddle Anesthesia,” bowel/bladder incontinence, and severe bilateral leg weakness. This is caused by a massive central disc herniation compressing multiple roots.
- Heel vs. Toe: Remember L5 = Heel (dorsiflexion) and S1 = Toe (plantar flexion). If they can’t stand on their tiptoes, think S1.
Activity: Radiculopathy Diagnostic Match
Memory Hooks:
L4: 4 kicks the door (Knee extension/Patellar). L5: 5 points to heaven (Dorsiflexion/Top of foot). S1: 1 stands on the Sun (Plantar flexion/Sole/Achilles).
You must be logged in to post a comment.