Learning Objectives
By the end of this session, the learner will be able to describe the anatomical components of the basal ganglia and their ipsilateral organization, explain the concept of disinhibition in the direct and indirect pathways, differentiate D1 vs D2 receptor modulation by dopamine, correlate lesions with hypokinetic vs hyperkinetic disorders, and identify key features and treatments of major movement disorders.
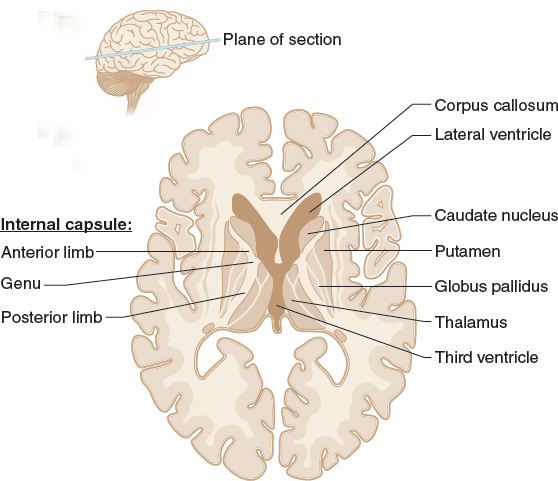
1. Structural Neuroanatomy
The basal ganglia initiate and regulate voluntary movement. Key Principle: All basal ganglia circuits are ipsilateral to the cortex.
| Structure | Sub-components | Origin |
|---|---|---|
| Striatum | Caudate nucleus + Putamen | Telencephalon |
| Globus Pallidus | External (GPe), Internal (GPi) | Telencephalon |
| Substantia Nigra | Pars compacta (SNpc), Pars reticulata (SNpr) | Midbrain |
| Subthalamic Nucleus | N/A | Diencephalon |
2. Pathway Physiology & Disinhibition
Both pathways rely on GABAergic inhibition and ultimately influence the motor cortex via the thalamic VL nucleus.
| Feature | Direct Pathway (Promotion) | Indirect Pathway (Suppression) |
|---|---|---|
| Mechanism | Cortex → Striatum → inhibits GPi → disinhibits Thalamus | Striatum → inhibits GPe → disinhibits STN → activates GPi → inhibits Thalamus |
| Dopamine | D1 → Excites pathway | D2 → Inhibits pathway |
| Acetylcholine | Minimal role | Activates the indirect pathway |
| Net Effect | ↑ Movement (facilitation) | ↓ Movement (suppression) |
Core Concept:
Movement is controlled by disinhibition — inhibiting an inhibitor results in activation.
3. Clinical Correlate: Movement Disorders
Disorders arise from an imbalance between the direct and indirect pathways.
A. Direct Pathway Lesions (Hypokinetic)
Reduced cortical stimulation → decreased movement
| Condition | Pathology | Clinical Features & Treatment |
|---|---|---|
| Parkinson Disease | Loss of DA neurons in SNpc; Lewy bodies (α-synuclein) | Pill-rolling tremor, rigidity, masked facies, bradykinesia, festinating gait Rx: Levodopa, anticholinergics |
B. Indirect Pathway Lesions (Hyperkinetic)
Excess cortical activity → increased involuntary movement
| Condition | Pathology | Key Features |
|---|---|---|
| Huntington Disease | CAG repeat (Chr 4); Caudate degeneration | Chorea, dementia, behavioral changes, anticipation |
| Hemiballismus | Lesion of contralateral STN | Violent, flinging limb movements |
| Wilson Disease | Copper accumulation; Putamen damage | Wing-beating tremor, Kayser-Fleischer rings, liver disease Rx: Penicillamine |
| Dystonia | Basal ganglia dysfunction | Sustained muscle contractions (e.g., torticollis) |
| Tourette Syndrome | Dopamine dysregulation | Motor & vocal tics are associated with OCD, ADHD |
Clinical Pearls:
- Disinhibition Rule: The basal ganglia work by inhibiting inhibitors — this is the key to understanding all pathways.
- D1 vs D2 Mnemonic:
- D1 = Direct = Do movement
- D2 = Indirect = Don’t move
- STN Lesion: Think “Ballistic” → Hemiballismus
- Caudate Atrophy: Classic for Huntington’s disease (seen on imaging)
- ↓ Dopamine → Parkinson’s → Hypokinetic
- ↓ Indirect pathway activity → Hyperkinetic disorders
You must be logged in to post a comment.