Learning Objectives
Differentiate between Myasthenia Gravis (MG) and Lambert-Eaton Myasthenic Syndrome (LEMS) based on their unique immunologic targets. Master the clinical “rules of thumb” regarding muscle use, reflexes, and associated malignancies (Thymic vs. Lung).
1. Comparison of NMJ Disorders
While both conditions present with proximal muscle weakness, their pathophysiology occurs on opposite sides of the synaptic cleft, leading to distinct clinical behaviors.
| Feature | Myasthenia Gravis (MG) | Lambert-Eaton (LEMS) |
|---|---|---|
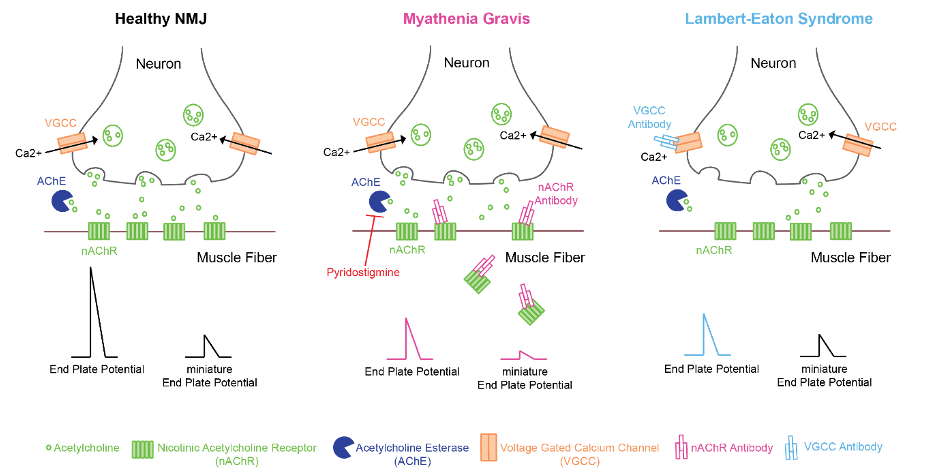
| Pathophysiology | Autoantibodies to postsynaptic ACh receptors. | Autoantibodies to presynaptic voltage-gated Ca2+ channels. |
| Mechanism | ACh receptor destruction/blockade. | Reduced ACh release (L comes before M). |
| Muscle Use | Worsens with use (fatigable). | Improves with use (potentiation). |
| Reflexes | Normal / Spared. | Hyporeflexia or absent. |
| Autonomic Sx | None. | Dry mouth, constipation, impotence. |
| Associated With | Thymoma, thymic hyperplasia. | Small cell lung cancer (SCLC). |
2. Clinical Presentation Details
MG often begins with ocular symptoms, whereas LEMS is more likely to present as a paraneoplastic syndrome in a patient with a smoking history.
- Myasthenia Gravis: Often presents with ptosis and diplopia. Bulbar involvement (dysphagia/difficulty chewing) is a major concern.
- Lambert-Eaton: Weakness is typically in the legs first. Improvement occurs because repeated stimulation “forces” more calcium into the presynaptic terminal.
Activity: NMJ Pathophysiology Flowchart Mapping
High-Yield Mnemonics:
- L vs M: Lambert-Eaton is Limbs (starts in legs) and Lungs (SCLC). Myasthenia is Mouth/Eyes (bulbar/ocular).
- The Alphabet Rule: L (Lambert) comes before M (Myasthenia), just as Presynaptic comes before Postsynaptic.
- Reflexes: Lambert = Low reflexes. Myasthenia = Maintained reflexes.
You must be logged in to post a comment.