Learning Objectives
Identify the multi-organ manifestations of IgG4-related disease (IgG4-RD) as a unified fibroinflammatory condition. Master the classic triad of elevated serum IgG4, lymphoplasmacytic infiltration, and storiform fibrosis across various anatomical sites.
1. Pathophysiology & General Features
IgG4-related disease is an immune-mediated spectrum of conditions. While it can mimic many malignancies or infections, it is defined by specific histopathological and serological findings regardless of the organ involved.
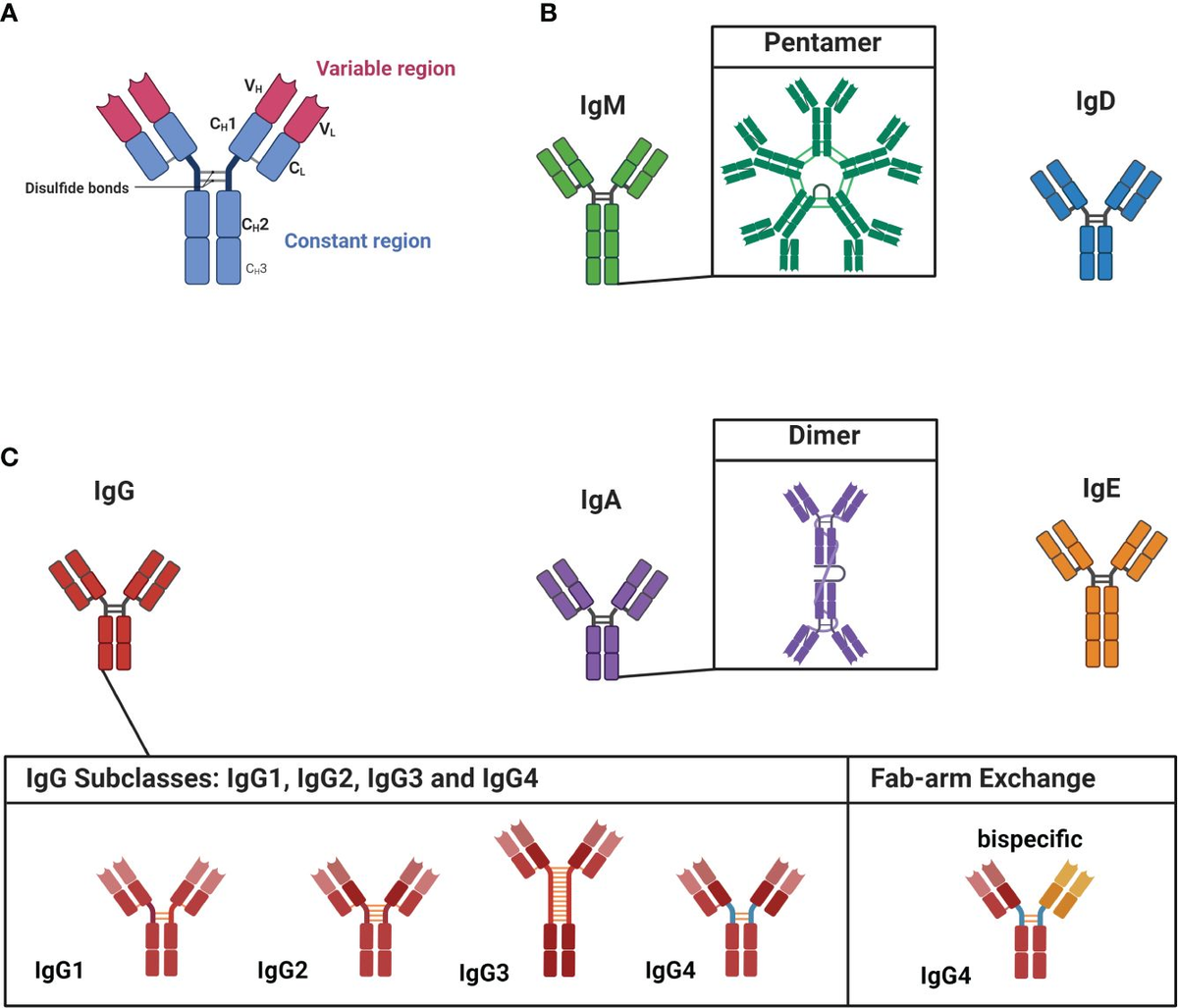
- Serum Findings: Most patients (though not all) demonstrate elevated serum IgG4 levels.
- Histology: Characterized by a dense lymphoplasmacytic infiltrate (rich in IgG4+ plasma cells) and storiform fibrosis (a “woven” appearance of collagen).
- Clinical Appearance: Often presents as a tumor-like swelling or mass in the affected organ.
2. Most Common Clinical Manifestations
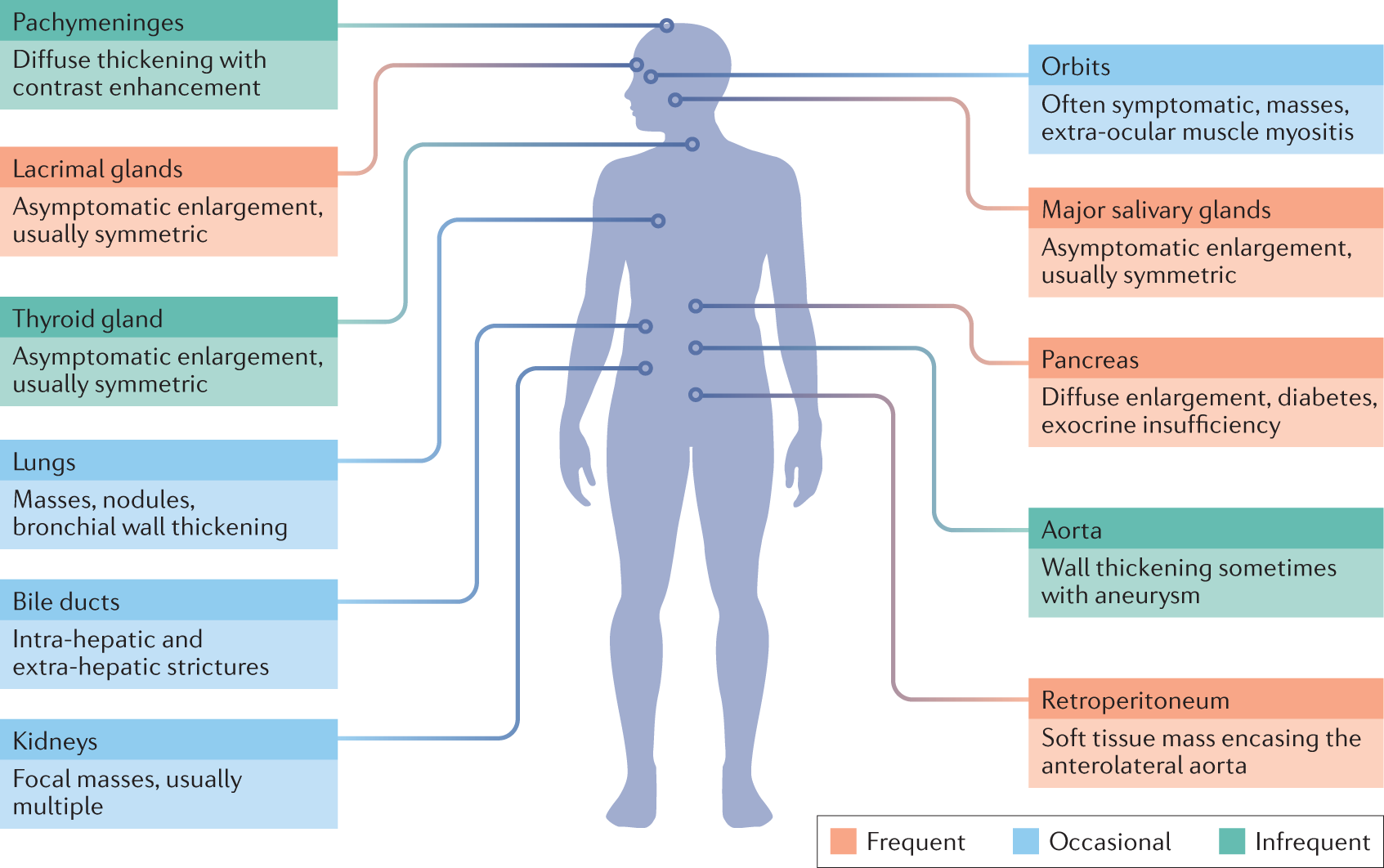
This “great masquerader” can affect almost any system, but certain classic presentations are highly testable.
| Organ System | Specific IgG4-Related Condition |
|---|---|
| Exocrine Glands | Sialadenitis (salivary) and Dacryoadenitis (lacrimal). |
| Thyroid | Riedel Thyroiditis (rock-hard, fixed thyroid). |
| Pancreas | Autoimmune Pancreatitis (Type 1) often presents as a painless mass. |
| Vasculature | Autoimmune Aortitis (can lead to TAA or AAA). |
| Retroperitoneum | Retroperitoneal Fibrosis (can encase ureters  hydronephrosis/AKI). hydronephrosis/AKI). |
Activity: IgG4-RD Organ Manifestation Mapping
High-Yield Mnemonics & Points:
- The “Hard” Disease: IgG4-RD causes fibrosis—think of “hard” organs like Riedel’s thyroid or a “rock-like” pancreas mass.
- Ureter Warning: If a patient has an unexplained AKI and an abdominal mass near the aorta, think Retroperitoneal Fibrosis.
- Treatment: These conditions are typically very steroid-responsive, which helps differentiate them from true malignancy.
You must be logged in to post a comment.