Learning Objectives
Identify the clinical diagnostic criteria for Fibromyalgia, focusing on chronic widespread pain and “tender points.” Differentiate Fibromyalgia from inflammatory conditions by recognizing its normal laboratory profile. Understand the multimodal treatment approach involving exercise and neuromodulators.
1. Clinical Presentation & Epidemiology
Fibromyalgia is a disorder of central pain processing (central sensitization) rather than a primary autoimmune or inflammatory disease. It most commonly affects females between 20 and 50 years old.
- Widespread Pain: Chronic musculoskeletal pain affecting both sides of the body, above and below the waist, for at least 3 months.
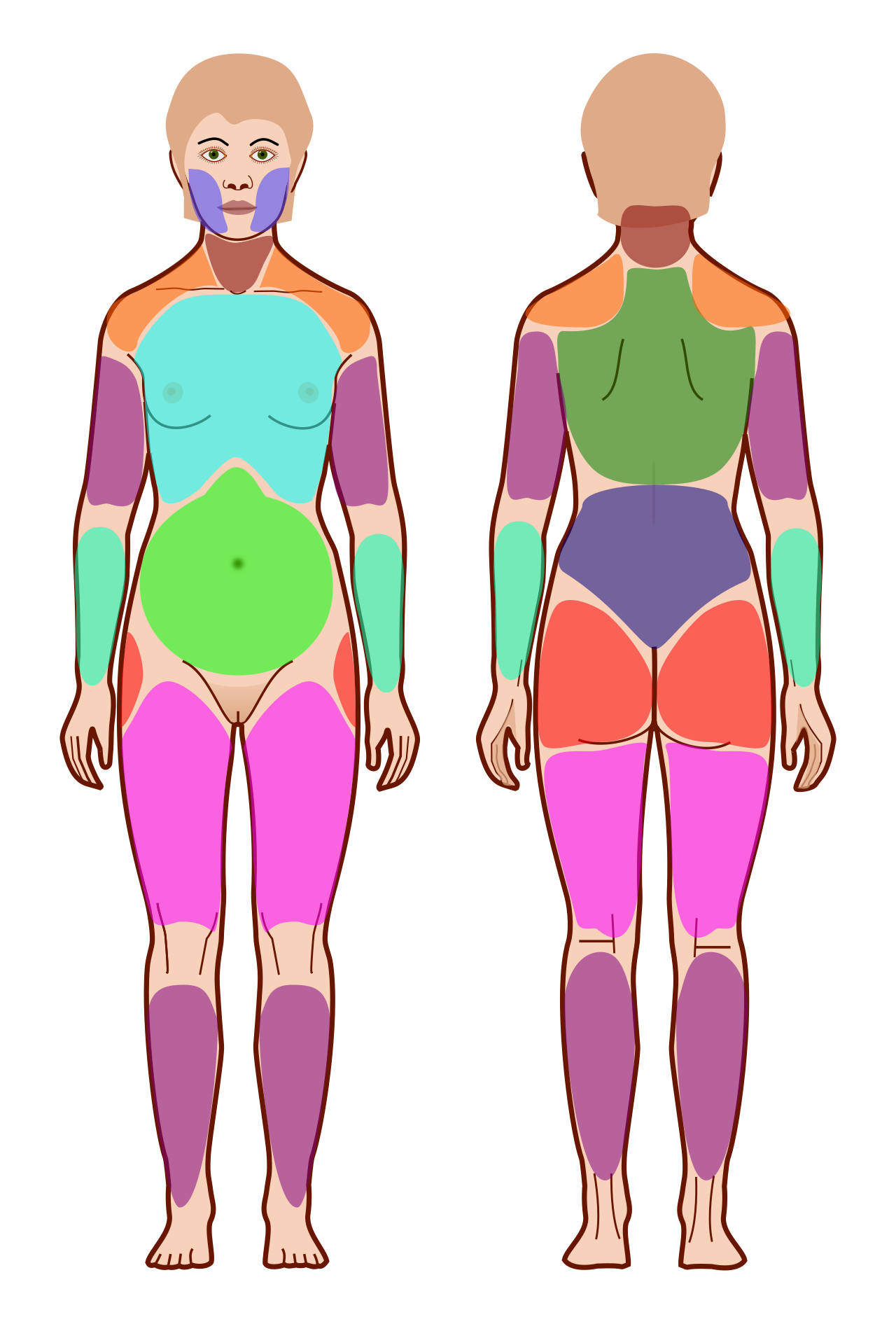
- Tender Points: Specific anatomical locations (e.g., mid-trapezius, lateral epicondyle, greater trochanter) that are painful to palpation.
- Associated Features:
- Fatigue & Poor Sleep: Patients often wake up feeling unrefreshed (“non-restorative sleep”).
- Paresthesias: Numbness or tingling without a dermatomal distribution.
- “Fibro Fog”: Cognitive disturbances, including poor concentration and memory loss.
2. Findings & Diagnosis
Fibromyalgia is often a “diagnosis of exclusion.” The most high-yield fact for exams is the absence of objective inflammatory markers.
| Test | Finding in Fibromyalgia | Clinical Significance |
|---|---|---|
| ESR / CRP | Normal | Rules out PMR and other inflammatory arthritides. |
| Creatine Kinase (CK) | Normal | Rules out myositis. |
| Biopsy | Normal | No evidence of muscle or nerve pathology. |
Activity: Differential
High-Yield Mnemonics & Treatment:
- The “Everything” Pain: If the vignette lists pain, fatigue, and normal labs, think Fibromyalgia.
- Management:
- Non-Pharm: Regular aerobic exercise (Gold Standard).
- Pharm: Antidepressants (TCAs like Amitriptyline, SNRIs like Duloxetine) and Gabapentinoids (Pregabalin).
You must be logged in to post a comment.