Learning Objectives
Differentiate between primary and secondary Antiphospholipid Syndrome (APS). Identify the clinical hallmarks of thrombosis and recurrent pregnancy loss, and master the laboratory paradoxes, such as the prolonged PTT and false-positive VDRL.
1. Pathogenesis & Clinical Criteria
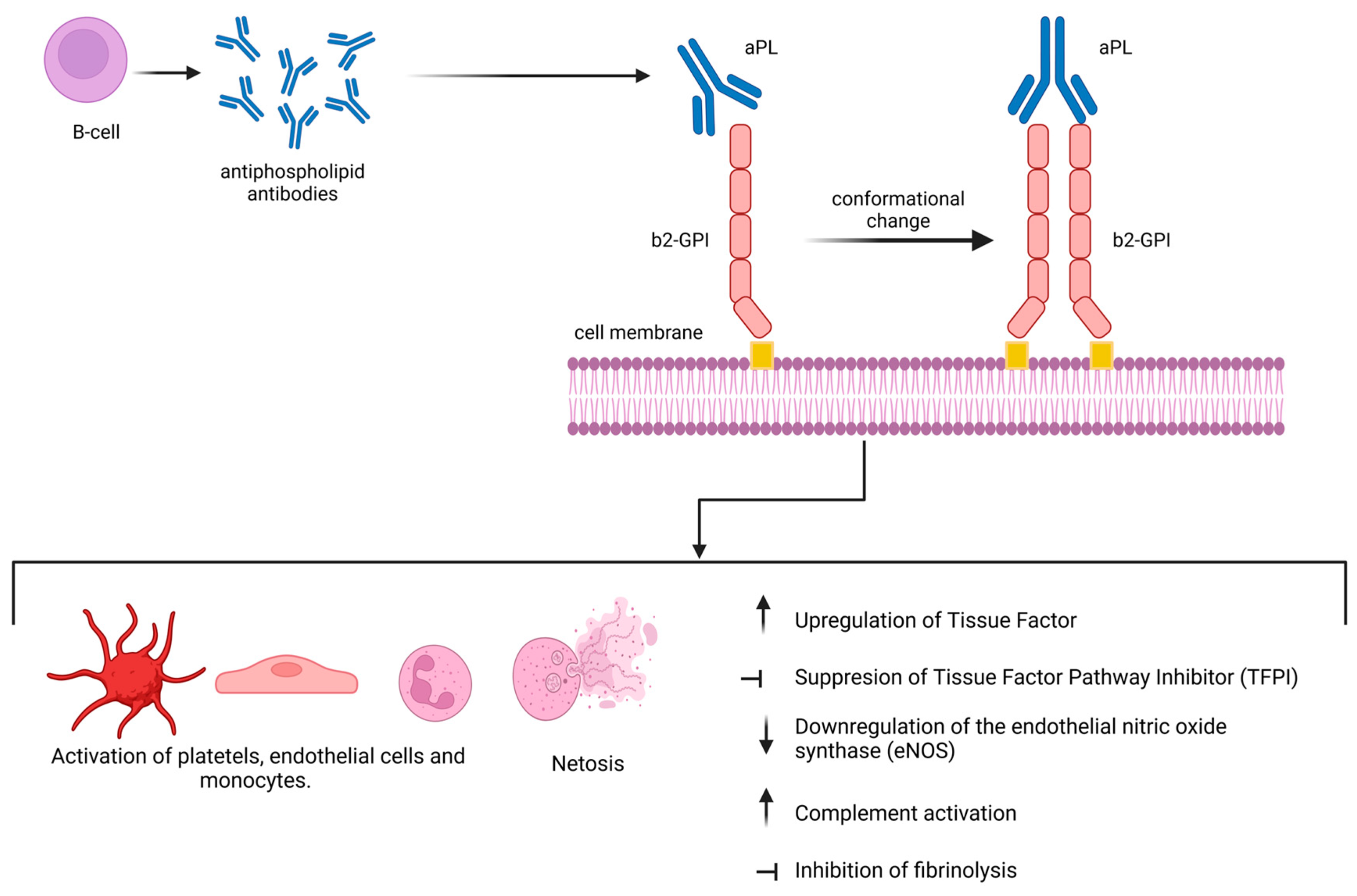
Antiphospholipid Syndrome (APS) is a systemic autoimmune disorder characterized by a “hypercoagulable state.” It can be a primary disorder or secondary to other autoimmune conditions, most commonly SLE.
- Clinical History: Diagnosis requires at least one clinical event:
- Thrombosis: Any history of arterial or venous thromboembolism (e.g., DVT, PE, Stroke).
- Obstetric Complications: Recurrent miscarriages (abortions) or unexplained fetal death.
- Treatment: Requires long-term systemic anticoagulation (e.g., Warfarin) to prevent further clotting events.
2. Laboratory Findings & Paradoxes
APS is well known in medical board exams for laboratory findings that appear contradictory to the patient’s clinical state.
| Lab Finding | Explanation / High-Yield Note |
|---|---|
| Lupus Anticoagulant | Causes a prolonged PTT in vitro. Paradoxically, the patient is pro-thrombotic (clotting) in vivo. The PTT does not correct with a 1:1 mixing study. |
| Anticardiolipin Antibodies | It can cause a false-positive VDRL/RPR (syphilis screen) because the test uses cardiolipin as an antigen. |
Anti- Glycoprotein I Glycoprotein I |
One of the three required diagnostic antibodies for APS. |
Activity: Interpreting the Mixing Study – APS vs. Factor Deficiency
High-Yield Mnemonics:
- The APS Paradox: “Long PTT in the lab, but Big Clots in the patient.”
- False Syphilis: “If the VDRL is positive but the FTA-ABS is negative in a woman with clots, think APS.”
- Secondary APS: Always screen for SLE in a young female with new-onset thrombosis.
You must be logged in to post a comment.