Learning Objectives
Differentiate Gout from Pseudogout based on crystal morphology and clinical triggers. Identify the biochemical mechanisms of hyperuricemia, specifically underexcretion versus overproduction. Master the pharmacological distinction between acute flare management and chronic urate-lowering therapy.
1. Pathogenesis of Hyperuricemia
Gout is an acute inflammatory monoarthritis caused by the precipitation of monosodium urate (MSU) crystals in joints. It is driven by hyperuricemia, which occurs via three primary mechanisms:
- Underexcretion (90%): Often idiopathic or due to renal failure. Exacerbated by thiazide diuretics.
- Overproduction (10%): Associated with high cell turnover (e.g., Tumor Lysis Syndrome), Lesch-Nyhan syndrome, or PRPP excess.
- Combined Mechanism: Alcohol use and von Gierke disease. Alcohol metabolism increases lactate, which competes with uric acid for excretion in the kidney.
Crystal Characteristics
The diagnosis is confirmed by synovial fluid analysis under polarized light. Monosodium urate crystals exhibit negative birefringence.
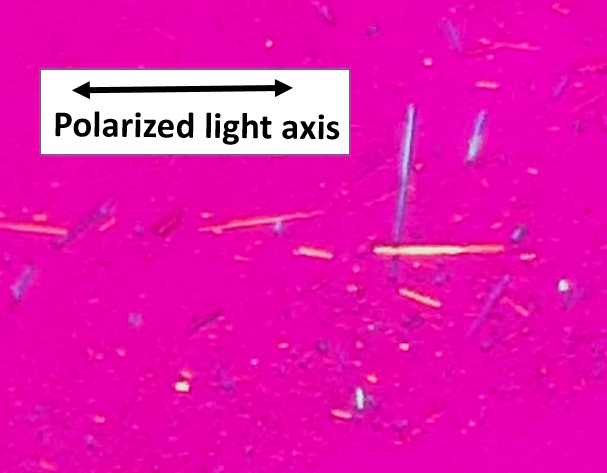
| Light Orientation | Color Finding |
|---|---|
| Parallel to the compensator axis | Yellow |
| Perpendicular to the compensator axis | Blue |
2. Clinical Symptoms & Presentation
Gout typically presents as an asymmetric, red, swollen, and exquisitely painful joint. Common triggers include purine-rich foods (red meat, seafood), trauma, or alcohol consumption.
- Podagra: Severe pain and inflammation of the 1st MTP joint of the big toe.
- Tophi: Chronic uric acid deposits are often found on the external ear, olecranon bursa, or Achilles tendon.

3. Treatment of Gout
| Phase | Medications | Mechanism/Note |
|---|---|---|
| Acute Attack | NSAIDs (Indomethacin), Glucocorticoids, Colchicine. | NSAIDs/Steroids reduce inflammation. Colchicine inhibits microtubule polymerization. |
| Chronic (Prophylactic) | Allopurinol, Febuxostat, Probenecid. | Xanthine oxidase inhibitors (Allopurinol) for overproducers. Probenecid for underexcretors. |
Activity: Gout vs. Pseudogout Crystal Challenge
- Crystal Color: “When the sticks are Laying (parallel), they are Yellow” (Low Yellow).
- Treatment: Allopurinol for Always (Chronic), NSAIDs for Now (Acute).
You must be logged in to post a comment.