Learning Objectives
- Differentiate between Osteomalacia (adults) and Rickets (children).
- Explain the pathophysiology of defective mineralization due to Vitamin D deficiency.
- Analyze the biochemical profile (Ca2+, PO4, PTH, ALP) in these conditions.
- Identify the classic radiographic and physical exam findings (e.g., Rachitic Rosary, Looser zones).
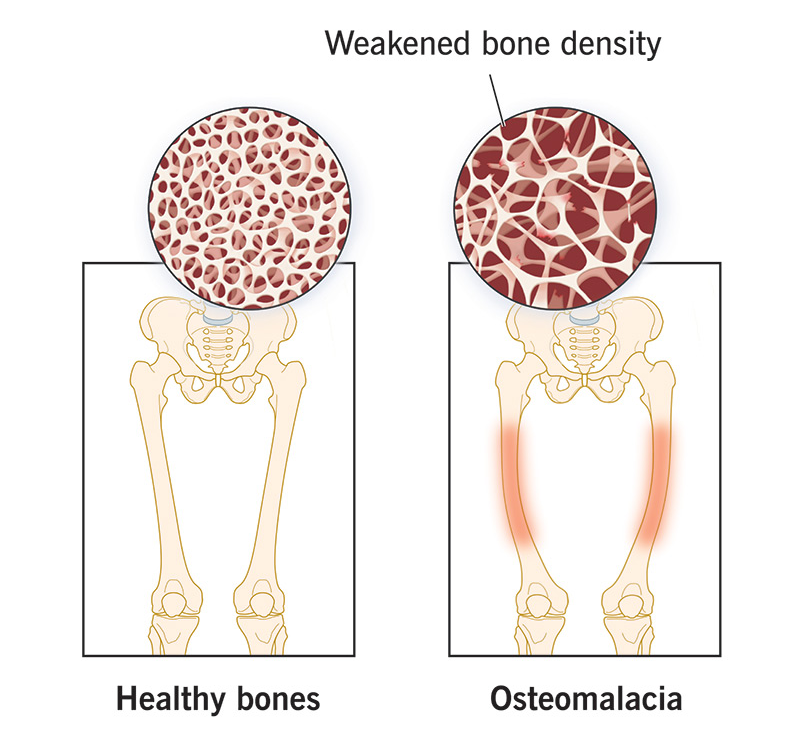
1. Pathophysiology: Softening of the Bone
Both conditions involve a failure of bone mineralization. The fundamental problem is that there is plenty of osteoid (the organic bone matrix), but it cannot be hardened with calcium and phosphate.
- Rickets (Children): Affects the epiphyseal growth plates. Because the plates are still open, the failure of mineralization leads to severe skeletal deformities.
- Osteomalacia (Adults): Affects the remodeled bone. Since the growth plates are closed, it presents as generalized bone softening and pain rather than structural bending of the limbs.
- Primary Cause: Most commonly due to Vitamin D deficiency (caused by malabsorption, poor diet, lack of sunlight, or chronic kidney disease).
2. Clinical & Radiographic Findings
| Finding | Description |
|---|---|
| Genu Varum | Bow legs: the soft weight-bearing bones of the legs bend outward in children. |
| Rachitic Rosary | Bead-like expansion of the costochondral junctions on the chest wall. |
| Craniotabes | Softened thinning of the skull bones in infants. |
| Looser Zones | Also called pseudofractures; radiolucent lines on X-ray that represent unmineralized osteoid (common in osteomalacia). |
3. Biochemical Profile (High Yield)
Understanding the compensatory mechanisms of the body is key to answering Step 1 questions on these topics.
Vitamin D: The root cause.
PTH: Low Calcium triggers the parathyroid glands to secrete PTH (Secondary Hyperparathyroidism).
Clinical Notes & Step 1 Pearls:
- Mineralization Lag: In osteomalacia, the “mineralization lag time” increases, meaning it takes much longer for osteoid to become bone.
- Metaphyseal Fraying: On X-ray of a child with rickets, look for “cupping and fraying” at the ends of the long bones.
- Vitamin D Pathway: Remember that the kidney is responsible for the final activation step (
). Chronic kidney disease is a major cause of secondary osteomalacia (Renal Osteodystrophy).
Activity: Mineralization Lab Challenge
Quick Mnemonics:
Osteomalacia: Think “M” for Mushy (Soft bones).
Rachitic Rosary: Think of a Religious Rosary (beads) on the Ribs.
Osteomalacia: Think “M” for Mushy (Soft bones).
Rachitic Rosary: Think of a Religious Rosary (beads) on the Ribs.
You must be logged in to post a comment.