Learning Objectives
- Trace the activation pathway of Vitamin D from skin/diet to the kidney.
- Identify the roles of PTH, Calcium, and Phosphate in regulating 1
-hydroxylase.
- Differentiate between Rickets and Osteomalacia.
- Explain the mechanism of Hypercalcemia in granulomatous diseases.
1. Synthesis and Activation
Vitamin D is unique because it can be synthesized endogenously via UV exposure or obtained through the diet. It requires two hydroxylation steps to become active.
- Source:
- D3 (Cholecalciferol): From sun exposure (stratum basale) and animal products (fish, milk).
- D2 (Ergocalciferol): From plants, fungi, and yeasts.
- Liver: Converts D2/D3 to 25-OH D3 (the primary storage form) via 25-hydroxylase.
- Kidney: Converts 25-OH D3 to 1,25-(OH)2 D3 (Calcitriol), the active form, via 1
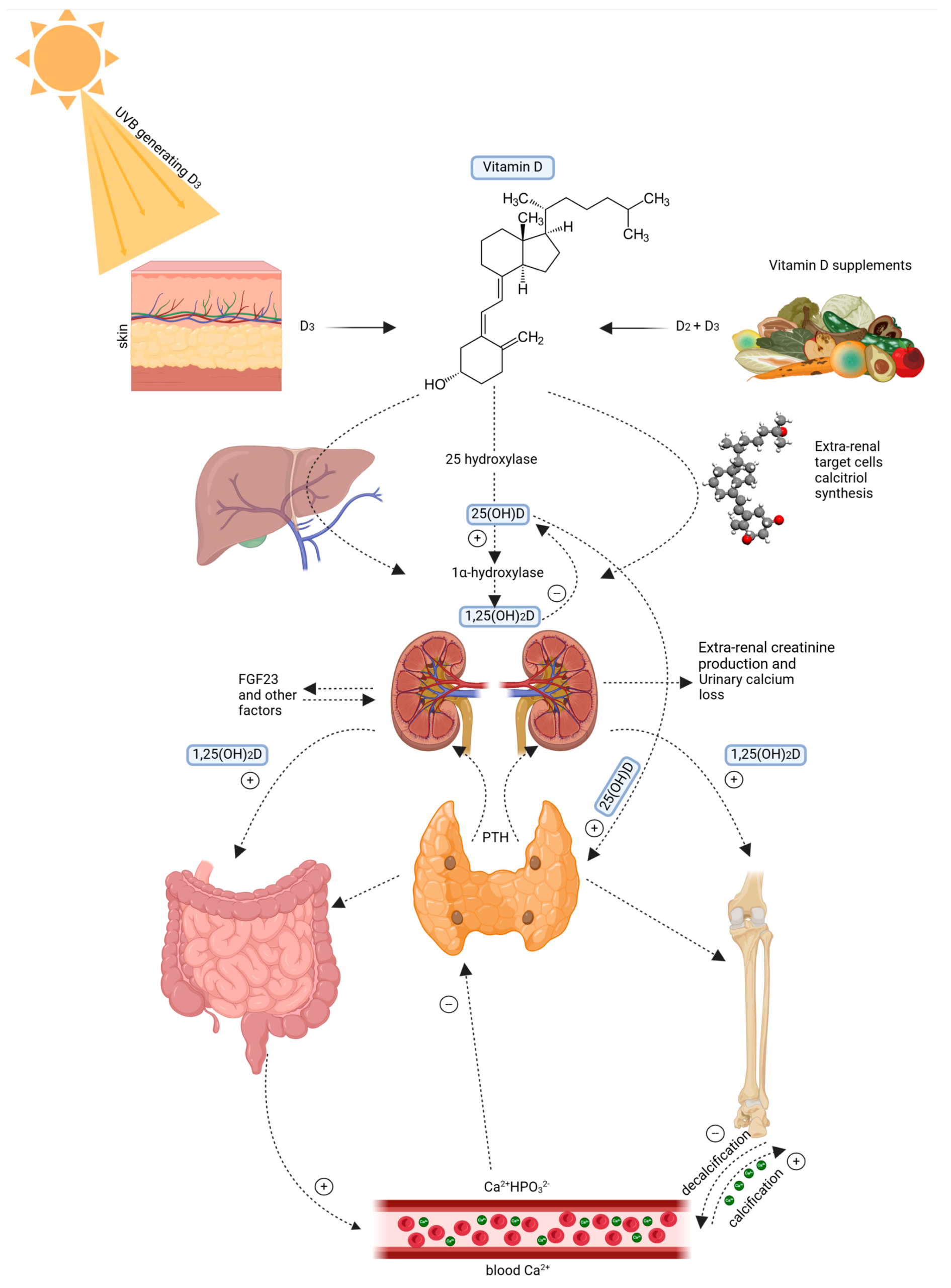
2. Physiological Functions & Regulation
Calcitriol acts primarily to increase serum calcium and phosphate levels to support bone mineralization.
| Target Organ | Action of 1,25-(OH)2 D3 |
|---|---|
| Intestine | ↑ absorption of dietary  and and  . . |
| Bone | ↑ mineralization (at low levels); ↑ resorption (at high levels). |
| Kidney | ↑ and reabsorption. |
Regulation: 1
3. Deficiency: Rickets and Osteomalacia
Deficiency leads to poor bone mineralization. Causes include CKD (loss of 1
- Rickets (Children): Softening of bones leading to skeletal deformities like genu varum (bowlegs) and rachitic rosary.
- Osteomalacia (Adults): Bone pain, muscle weakness, and increased risk of “pseudo-fractures.”
- Hypocalcemic Tetany: Involuntary muscle contractions due to low serum calcium.
4. Toxicity & Granulomatous Disease
Excess Vitamin D causes Hypercalcemia and hypercalciuria (loss of appetite, stupor).
High-Yield Correlation: In granulomatous diseases (like Sarcoidosis), epithelioid macrophages contain 1$\alpha$-hydroxylase and activate Vitamin D independent of PTH, leading to hypercalcemia.
Activity
You must be logged in to post a comment.