Learning Objectives
- Describe the role of Tetrahydrofolate (THF) in DNA and RNA synthesis.
- Distinguish B9 deficiency from B12 deficiency using neurological and laboratory markers.
- Identify common pharmacological antagonists of folate metabolism.
- Explain the clinical importance of folate in pregnancy and neural tube development.
1. Biochemistry and Function
Vitamin B9 (Folate) is converted into its active coenzyme form, Tetrahydrofolic acid (THF). THF is the primary carrier for 1-carbon transfer and methylation reactions.
- Synthesis: Crucial for the synthesis of nitrogenous bases (purines and thymidine) in DNA and RNA.
- Absorption: Occurs in the jejunum.
- Storage: Small reserve pool in the liver (lasts ~3–4 months).

2. Deficiency: Megaloblastic Anemia
Folate deficiency leads to impaired DNA synthesis, which manifests in rapidly dividing cells like hematopoietic precursors.
[Image of hypersegmented neutrophil in megaloblastic anemia]
| Clinical Finding | Details |
|---|---|
| Hematologic | Macrocytic, megaloblastic anemia; Hypersegmented PMNs (neutrophils with >5 lobes). |
| Neurologic | NO neurologic symptoms (this differentiates B9 from B12 deficiency). |
| Labs | ↑ Homocysteine, but Normal Methylmalonic Acid (MMA). |
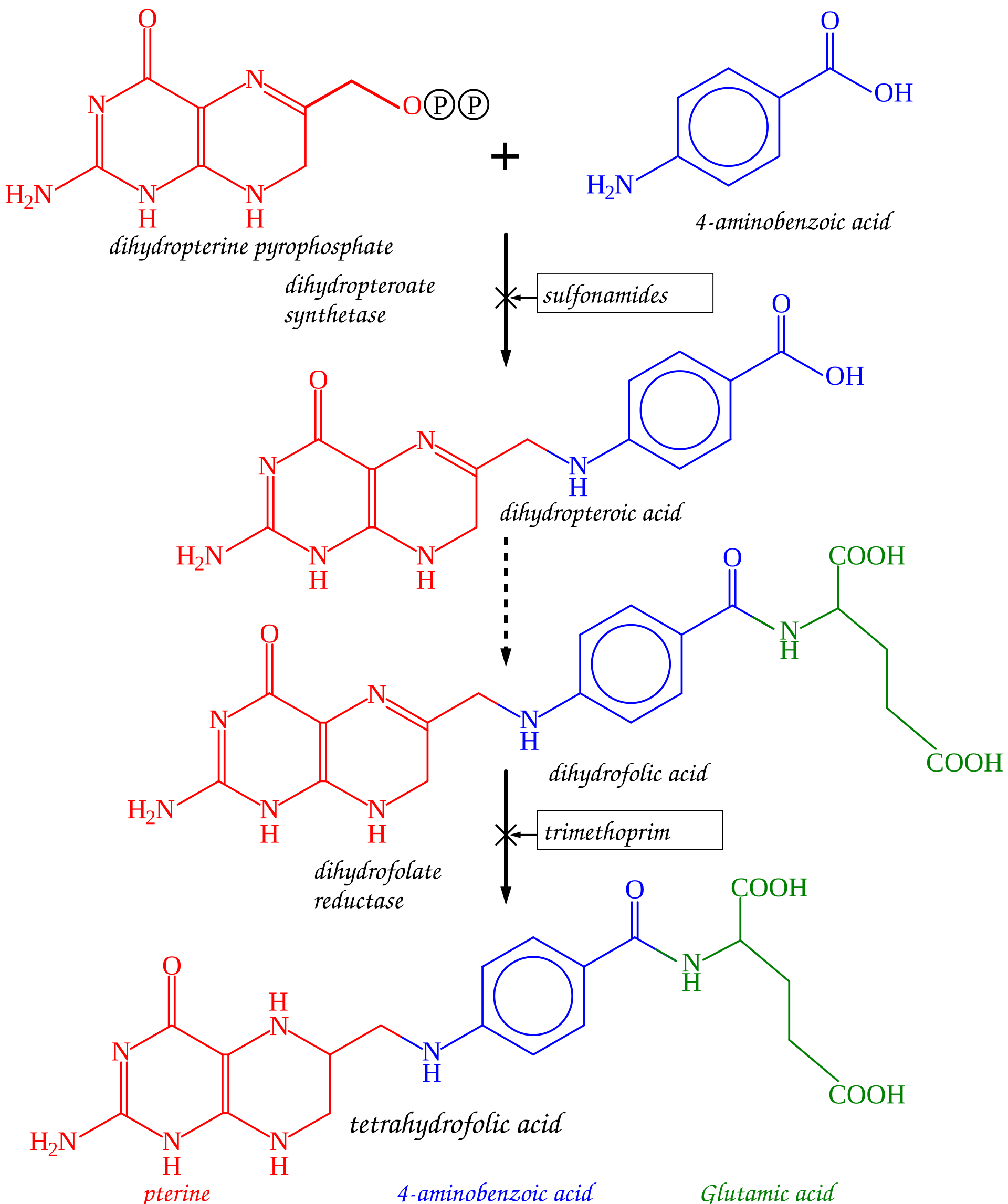
3. Pharmacological Antagonists
Several high-yield drugs interfere with folate metabolism and can precipitate deficiency:
- Methotrexate & Trimethoprim: Inhibit Dihydrofolate Reductase (DHFR).
- Phenytoin: Interferes with intestinal folate absorption.
4. Pregnancy and Neural Tube Defects
Low folate levels during the first weeks of pregnancy are a major risk factor for Neural Tube Defects (NTDs) such as spina bifida and anencephaly.
Protocol: Supplemental folic acid should be started at least 1 month before conception and continued through the 9 months of pregnancy.
Activity
You must be logged in to post a comment.